
Oxygen Therapy What is oxygen therapy? Oxygen is necessary for the survival and effective functioning of all body tissues. When body tissues are not receiving enough oxygen, we have to supplement...
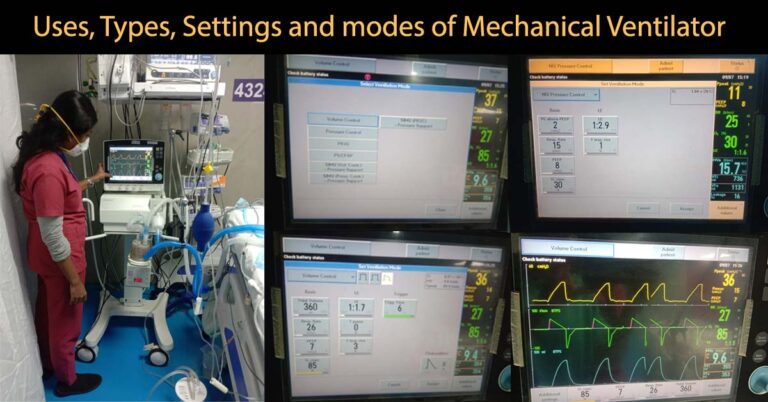
What is a Mechanical ventilator? A mechanical ventilator is a machine, which provides artificial ventilation when the patient’s normal ventilation mechanism fails (Gives artificial breath when patient...

What are Sleep disorders? Sleep Disorders are a group of conditions producing changes in the ability of a person to sleep well on regular basis. Sleep disorders can affect the overall health of the...

What is Capnography? Capnography is a clinical procedure used for the measurement of CO2 levels in respired air at the end of expiration (End tidal CO2). In Capnography the results are displayed in...
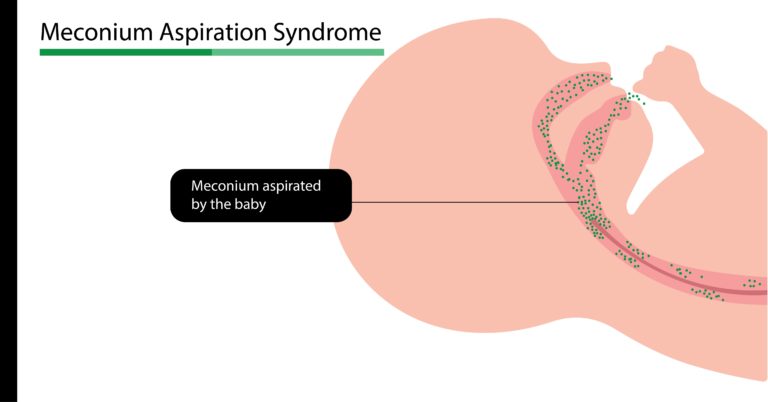
What is Mecomium Aspiration Syndrome? Meconium aspiration syndrome is a type of respiratory distress occurring in babies born with meconium stained amniotic fluid or aspirated meconium during...

What is Respiratory Distress Syndrome (RDS) in Neonates? RDS once called Hyaline Membrane Disease (HMD) or Surfactant deficiency syndrome (SDD) is mainly seen in premature babies and manifest within...

What is meant by Arterial Blood Gas analysis? An arterial blood gas analysis is a procedure (test) that is performed to measure oxygen, carbon dioxide and acid/base status (pH) in arterial blood. What...
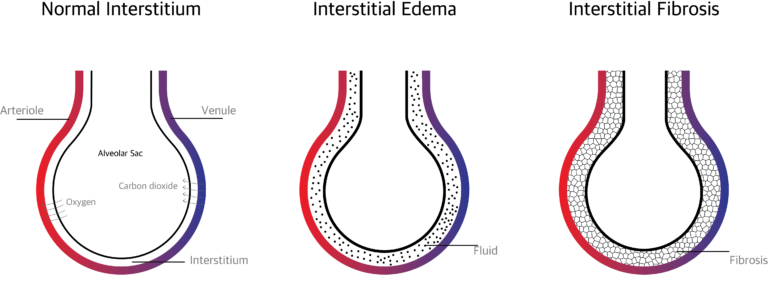
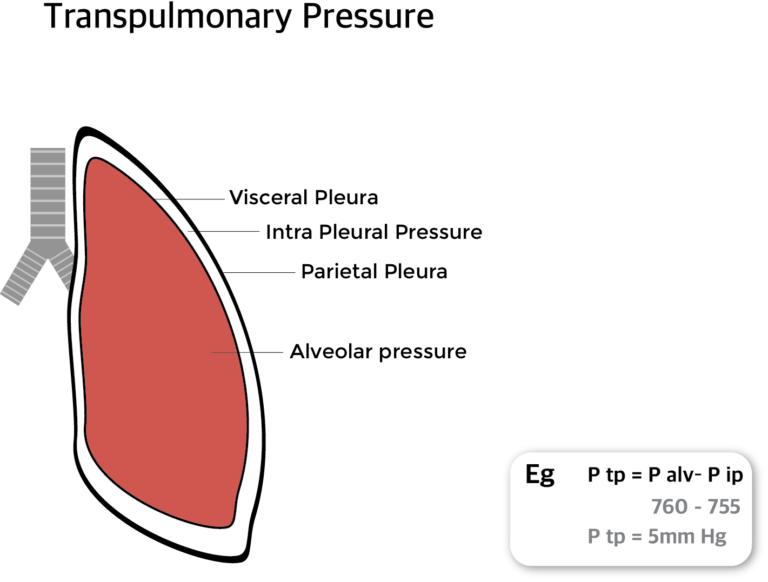
What is pulmonary Interstitium? The Pulmonary Interstitium is the anatomical space between the alveolar epithelial cells and the endothelium of the pulmonary capillaries. It continues as the space...
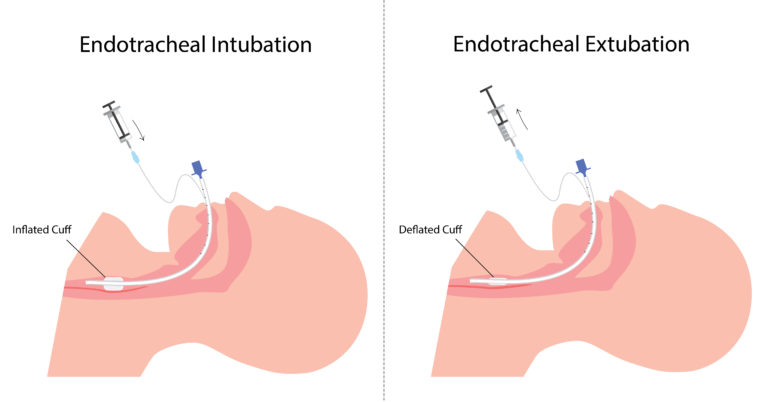
What is Tracheal Extubation? Endotracheal tube is a flexible polyvinyl chloride tube which helps to assist breathing. The process of placing endotracheal tube in the airway is called Intubation...
What is lung expansion therapy? Lung expansion therapy includes many techniques to improve pulmonary function by increasing alveolar recruitment (open collapsed alveoli) and airway clearance. It...
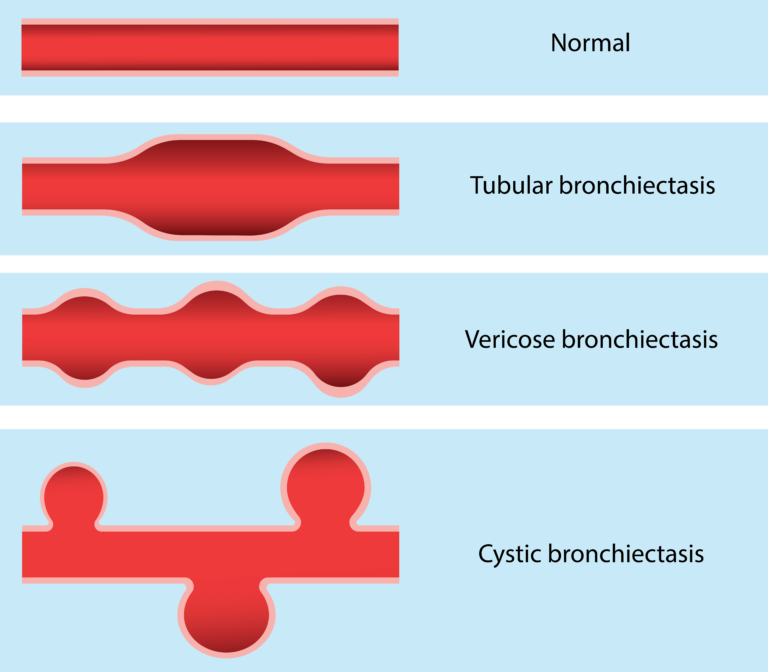
What is bronchiectasis? Bronchiectasis is an abnormal irreversible (permanent) dilatation of some bronchi or bronchioles (enlargement of parts of airway). What are the causes of bronchiectasis? The...
Who are called respiratory therapist? Respiratory therapist also called as respiratory care practitioners are paramedical professionals who basically deals with the problems related to lungs and...
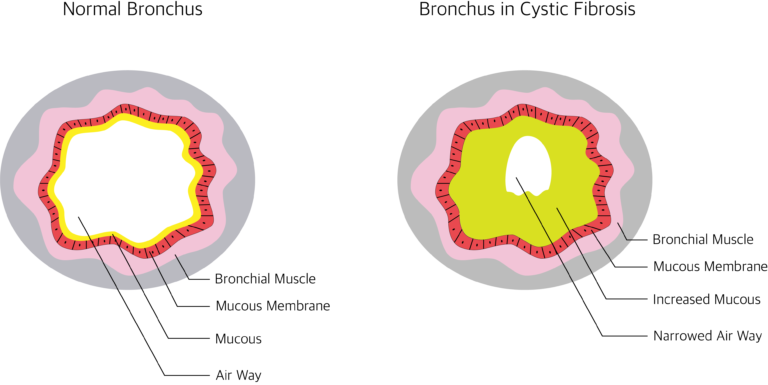
What is Cystic Fibrosis? Cystic Fibrosis is a hereditary disease caused by gene mutation (alteration in gene sequence and structure). The mutation occurs in the gene for the CFTR protein (cystic...
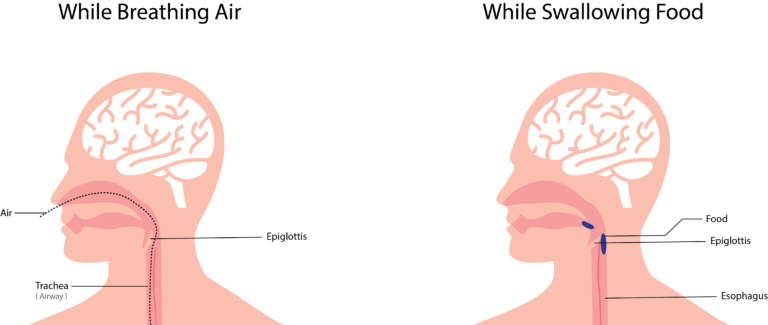
What is Epiglottis? Epiglottis is a leaf shaped soft bone (cartilage) at the base of the tongue. It is a flap like structure, which block the entry of food materials from entering the windpipe...

What is Intubation? Intubation ( Endotracheal Intubation ) is a process of placing a tube in the airway from the nose or mouth to trachea (wind pipe) to provide artificial respiration. Who may need...
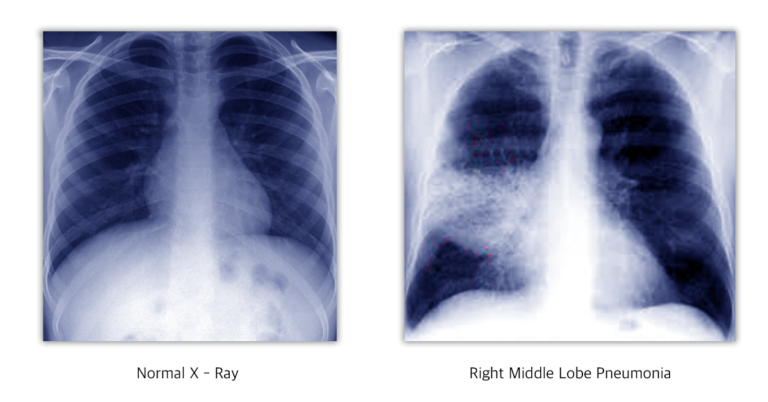
What is pneumonia? Pneumonia is the inflammation of the lung parenchyma ( tissue that involves in gas exchange in the lungs otherwise called alveolar tissue ). When inflammation is caused by infection...
Article written by Ravindran O.S & Aruna Mani Internet addiction Internet addiction is characterized by excessive use of the internet, and that is detrimental to the user. There exists no clear...

Dark circle under the eye Dark circle under the eye is one of the common cosmetic problems faced by both men and women. It may make them appear older and it gives them a hollowed –out look (ghost like...
SWINE FLU ( H1N1 Influenza) What is Swine Flu? Swine flu otherwise called as H1N1 Influenza is a contagious respiratory disease caused by the influenza virus of the type H1N1. Why it is called...

Excessive Yawning What is yawning? Yawning is a natural involuntary physiological action shown when people are tired or bored. Yawning involves opening the mouth widely, taking a long and deep breath...