What is Mecomium Aspiration Syndrome?
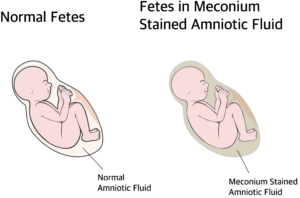
Meconium aspiration syndrome is a type of respiratory distress occurring in babies born with meconium stained amniotic fluid or aspirated meconium during delivery.
What is Meconium and how it is aspirated?
The term meconium refers to the sterile stool present in the fetal intestine. (earliest stool of the baby). Meconium contains epithelial cells of the intestine, lanugo (fetal hair), blood cells, bile, mucus, intestinal secretions and amniotic fluid. Meconium is thick, sticky, odorless and dark yellow to olive green in colour. Normally the child passes meconium hours after birth.
Passage of meconium is prevented by a low motilin level in the fetus. Motilin is a hormone (chemical) which controls motility of the intestine (peristalsis). Before delivery the motilin level will be low, preventing intestinal movements. Motilin is produced around 34 weeks of gestation. In full term and post dated babies the motilin level is high and when there is vagal stimulation by head or cord compression or stress inside uterus (hypoxia, acidosis etc) peristalsis increases and the anal sphincter is relaxed allowing meconium to come out.
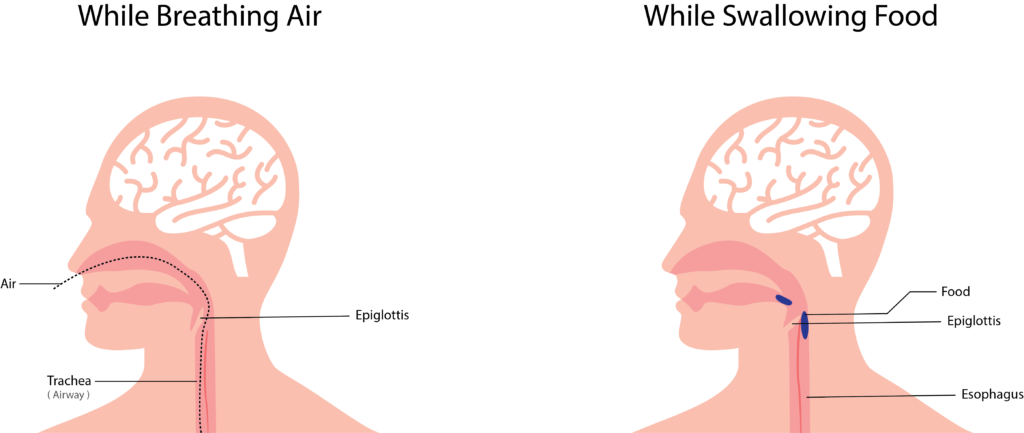
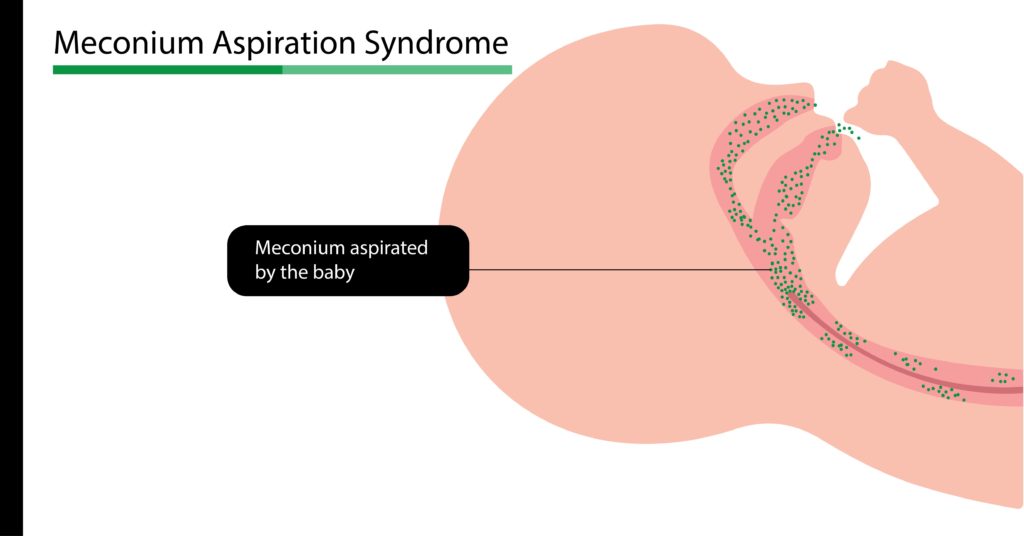
This may occur during or before the delivery. Since the fetus is surrounded by the meconium stained amniotic fluid, when the baby gasps, it is aspirated into the lungs, resulting in Meconium Aspiration Syndrome.
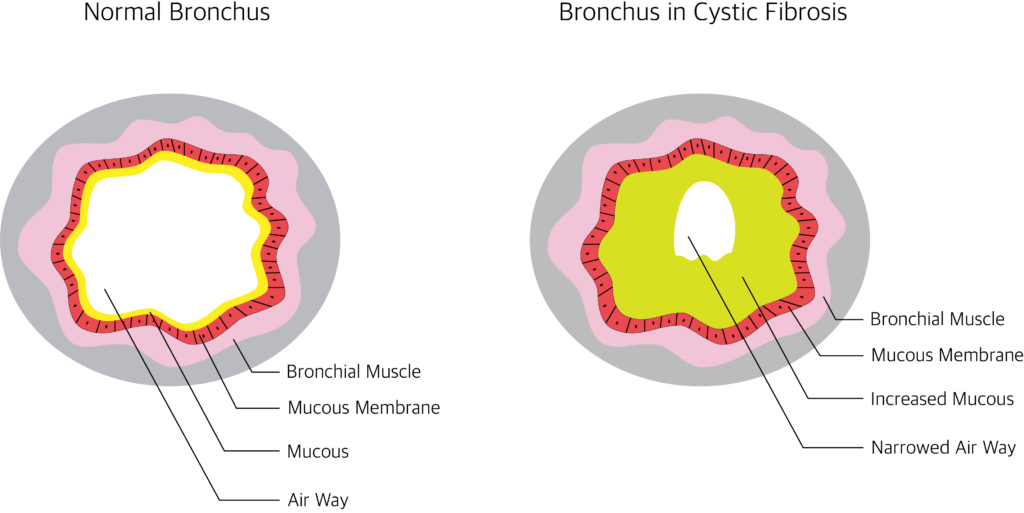
Even though it’s sterile, it causes inflammation and may mechanically obstruct the airway, inactivate surfactant, and prevent gas exchange. Meconium aspiration syndrome is commonly found in full-term (>39 weeks) or post dated deliveries.
Depending upon the amount and duration of aspiration, the newborn may show symptoms ranging from mild to life-threatening distress. Therefore treatment has to be started as soon as possible.
What are the predisposing factors of MAS?
Mother’s:
- Post-term pregnancy
- Prolonged, hard delivery
- Hypertension, diabetes, preeclampsia
- Mother smoking during pregnancy and maternal drug abuse.
Fetal:
- Infection or stress to the fetus
- Decreased oxygen supply
- Cord or head compression.
What are the clinical features of Meconium Aspiration Syndrome?
- Newborn may have yellow discoloration of the umbilical cord, nail bed and skin
- Increased respiratory rate and difficulty in breathing
- May use extra muscle for breathing normally
- May have grunting and nasal flaring
- The newborn may have bluish discoloration of lips, hands, and legs
- The newborn may also have box-shaped (barrel-shaped) chest
- Chest sound through auscultation reveals rales and ronchi,
- Meconium stain on body
- May show signs of post maturity like peeling skin and long finger nails.
Other diseases with similar clinical signs (differential diagnosis):
- Respiratory Distress syndrome
- Perinatal asphyxia
- Transient Tachypnea of the New Born
- Congenital Heart Disease
- Surfactant deficiency
- Pneumonia and sepsis of newborn
What are the tests done in Meconium Aspiration Syndrome?
X-ray chest
- Irregular, linear, streaky infiltrates.
- Hyper inflated lungs,
- Flat diaphragm.
Pulseoxymeter
To measure oxygen saturation and degree of shunting
The blood flow of the heart in the fetus is different from that of the newborn. There will be a flow of blood directly to the left side bypassing the pulmonary circulation due to high pulmonary pressure. But this becomes normal when the pulmonary pressure drops as the baby takes the first breath.
When this process is interrupted, the pressure remains high and may result in Persistent Pulmonary hypertension of Neonates. Due to this, there will be always a difference of at least 10 % SpO2 between right hand (higher than other) and other limbs.
Arterial blood gas analysis
Decreased oxygen and increased CO2, acidosis. Echocardiogram and ECG to rule out heart diseases.
Blood and aspirated meconium for culture and drug sensitivity testing.
How Meconium Aspiration Syndrome baby is managed?
As soon as the head is delivered, suction is applied to mouth, nose and pharynx. Soon after the delivery the baby’s vitals assessed.
If the baby is vigorous (active)
Heart rate above 100/minute, having spontaneous breathing, spontaneous movements and good tone provide supportive care with frequent monitoring. No tracheal suctioning or intubation necessary.
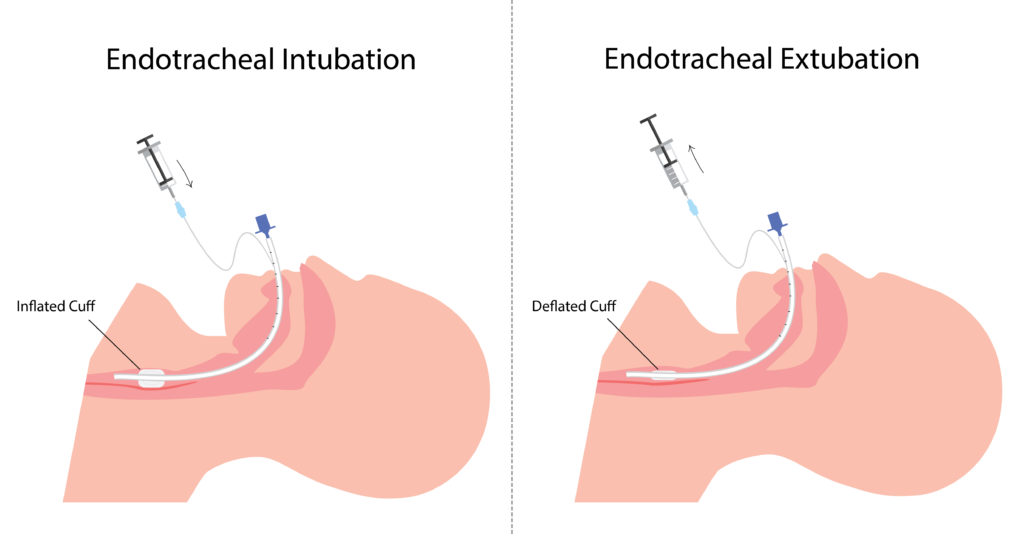
If the baby is not vigorous (limp)
Baby having cyanosis, increased respiratory rate, reduced heart rate and the baby is limp without spontaneous breathing, tracheal suctioning is done.
Neonatal intensive care given.
Oxygen therapy using simple oxy hood (transparent helmet-like hood) or Continuous Positive Airway Pressure (CPAP) through a mask, ECMO (Extracorporeal membrane oxygenation) or Mechanical ventilation can be started according to the severity of distress.
Empirical antibiotics to prevent infection
Nitric oxide inhalation to open blood vessels and prevent pulmonary hypertension.
Surfactant replacement therapy to replace the inactivated surfactant and open alveoli. Chest physiotherapy.
How to prevent Meconium aspiration Syndrome?
- Good antenatal, ante partum and intra partum care can prevent MAS.
- Mothers should avoid smoking and drug abuse.
- Avoid post dated delivery by induced labor.
- Suctioning the nose, mouth and pharynx before the delivery of shoulders
- If the amniotic fluid is stained with meconium, the amniotic fluid can be diluted by infusing isotonic liquid in to the uterus (Amnioinfusion).