
Oxygen Therapy


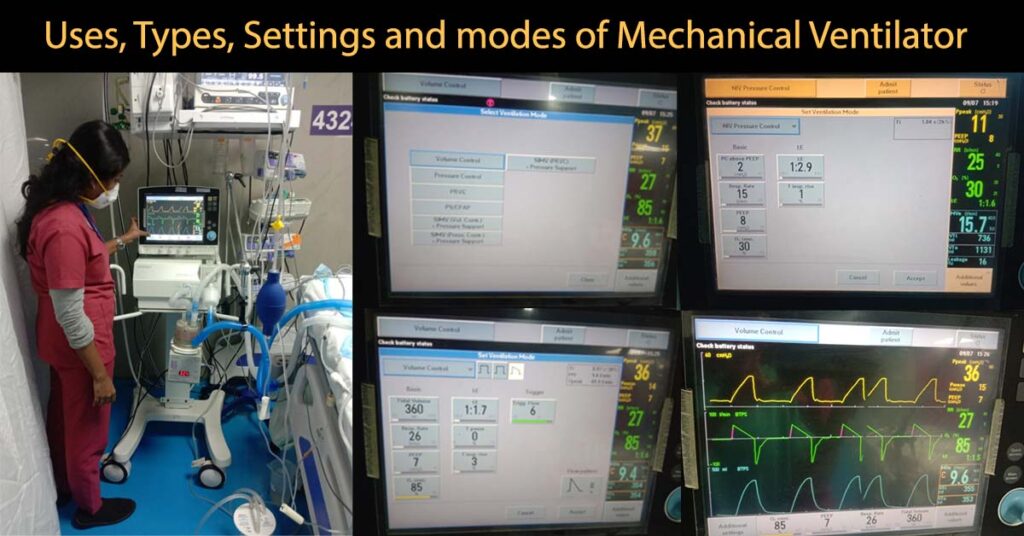
A mechanical ventilator is a machine, which provides artificial ventilation when the patient’s normal ventilation mechanism fails (Gives artificial breath when patient finds it difficult to breathe or unable to breathe on their own).
Ventilator provides oxygen and removes excess carbon dioxide (it acts as another lung).
Ventilators are of 4 basic types.
What is invasive ventilation?
In invasive ventilation air/oxygen is delivered through a tube placed inside the windpipe (Endo-tracheal intubation) or through Tracheostomy.
What is non-invasive ventilation?
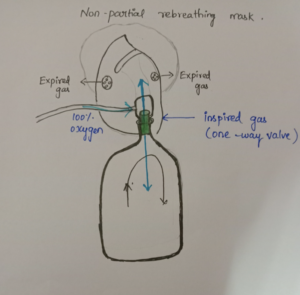
In Non-invasive ventilation air or oxygen is delivered via a face mask avoiding endo-tracheal intubation.
Basic display orders in ventilator settings:
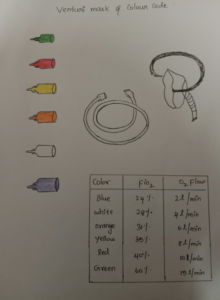
Amount of oxygen present in the inspired air.
Normal range (21%-100%).
complete one count of inspiration and expiration for one minute ( breathing rate ).
Respiratory rate is different for adults and neonates (newborns).
Normal Range of RR for adult: 12 – 16 breaths/minutes
Normal Range of RR for neonates: 40-60 breaths/minutes
Volume of air present during normal inspiration and expiration.
Normal range: 4 – 8 ml per kg body weight (approximately 500ml)
Pressure in the alveoli at the end of expiration. It prevents alveoli collapse.
Normal range: 5cmH2o – 10cmH2o.
Weaning is the gradual withdrawal of ventilator support. Weaning is started when the cause is treated successfully.
The common complications of mechanical ventilation are: airway trauma, airway malfunction, acid base disturbances, oxygen toxicity, arrhythmias, barotraumas, infection, pneumothorax etc.
Mechanical Ventilator Read More »

Sleep Disorders are a group of conditions producing changes in the ability of a person to sleep well on regular basis.
Sleep disorders can affect the overall health of the person, his quality of life and safety of the person while driving or working in daytime.
People spend more than one third of their life sleeping. Sleep allows our brain and body to rest and repair itself.
Sleep help in growth, improves memory, synthesize hormones, reduces stress, boost immunity, reduces inflammation, maintains healthy blood pressure and blood sugar levels, and prevent cancer.
This is the most common sleep disorder. Here the person develops difficulty in falling asleep and maintaining quality sleep.
Here the person develops abnormality in breathing while sleeping. Common sleep related breathing disorders are
Snoring: Harsh vibratory sound produced, when air passes through relaxed tissues of throat. Snoring can also occur in sinusitis, enlarged tonsils, cold, and in obesity.
Catatherenia: Moaning or groaning sound produced during expiration.
In parasomnia the person may have unwanted physical actions or experiences during sleep.
E.g.: Sleep walking, sleep talking, sleep terrors, sleep enuresis and nightmare disorder.
The person may have simple and repetitive movements during sleep.
E.g.: Restless leg syndrome, Periodic limb movement disorder and sleep bruxism.
Here the person may have desynchronization between his internal clock (sleep wake cycle) and light darkness cycle.
E.g.: Jet lag disorder and Shift work disorder.
Symptoms depend on the type of disorder. The person may take long time to sleep, may wake up frequently and may have difficulty in going back to sleep. May be drowsy and fall asleep at daytime. Snore and may stop breathing often during sleep. Move or jerk their arms and legs during sleep.

Polysomnography is the common sleep study done. It is done in a sleep lab or home. The person is made to sleep and activity of brain (EEG), oxygen saturation, Muscle movements (EMG) abdominal and leg movements, oral and nasal air flow and eye movements are recorded. Number of apnea and hypopnea are recorded.
MSLT is usually done in day time after polysomnography test. This test shows how quickly a person can fall asleep. In daytime the person is asked to lie down and try to sleep. Each nap time is 20 minutes. If the person sleeps he is awakened after 15 minutes. Test repeated after 2 hours, like that 5 tests are done in that day. Time of light out and sleep onset is called sleep latency Usually done to diagnose narcolepsy and hypersomnia.
Below 5 minutes – Sever sleepiness
5 to 10 minutes – Moderate sleepiness
10 to 15 minutes – Mild sleepiness
In MWT how well a person is able to stay awake is tested. In a dark, quit and comfortable room the person is asked to stay awake and not to fall asleep. MWT is also done after overnight polysomnography. Here also 20 minutes slots are given repeated every 2 hours.
Sleep Disorders: Causes, Diagnosis and Treatment Read More »
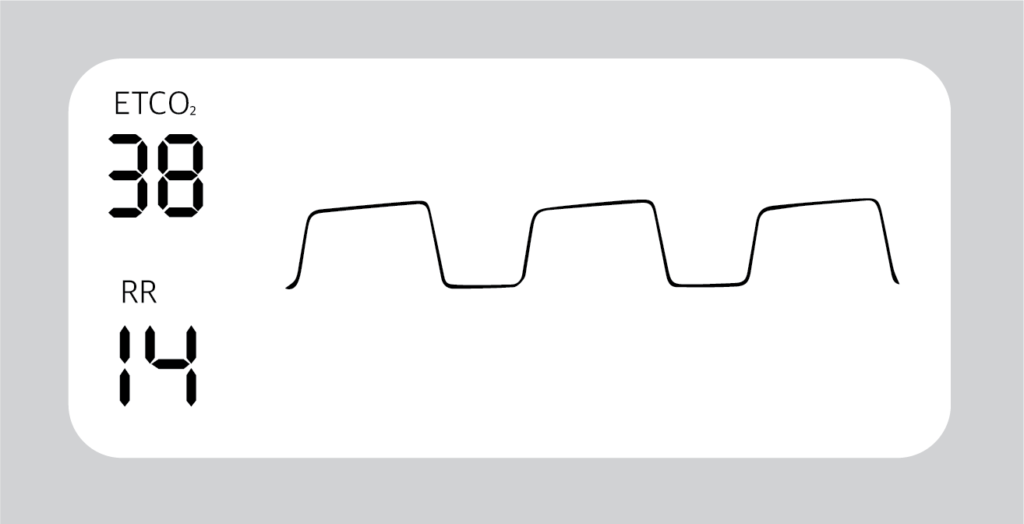
Capnography is a clinical procedure used for the measurement of CO2 levels in respired air at the end of expiration (End tidal CO2). In Capnography the results are displayed in graphic and numerical form.
Graphic form gives more details to diagnose and assess the ventilation of the patient.
Capnometry is also used to measure End Tidal CO2 but gives results only in numerical form. (only in numbers and no graphic form)
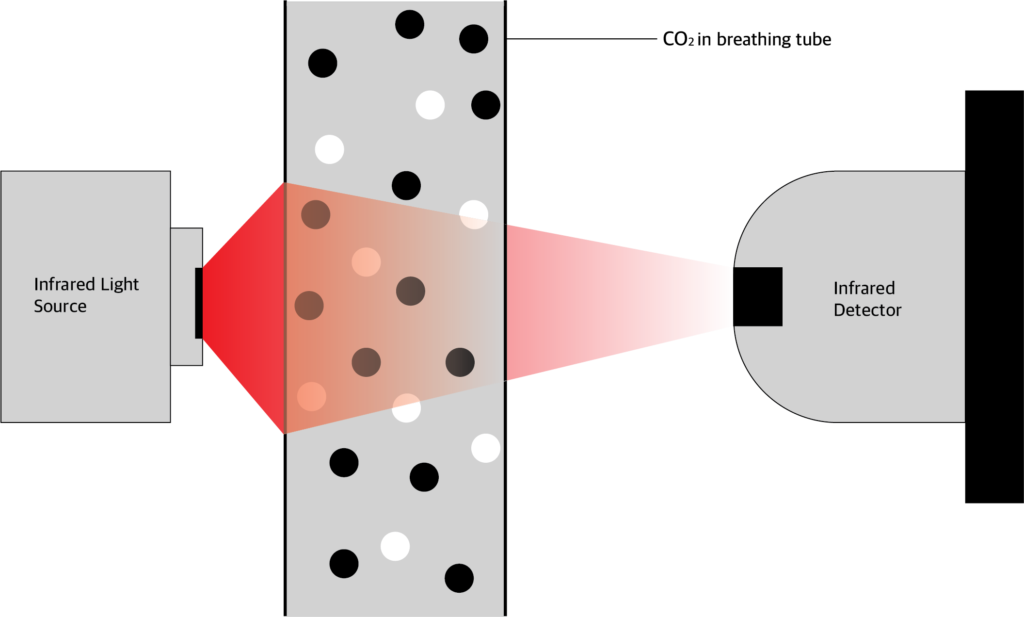
Carbon dioxide absorbs infrared light energy. The amount of infrared light absorbed depends on the CO2 concentration. In ccapnography device, CO2 is allowed to pass through infrared light.
The amount of light absorbed is calculated by comparing the amount of infrared light send from the source and the amount received by the photo detector.
From this the CO2 pressure is calculated and values given in graphic and numerical form.
Normal ETCO2 value is between 35 to 45 mmHg.
Normal respiratory rate is 14/min.
The mainstream analysier chamber placed between the endotracheal tube and the ventilator circuit.
Advantages:
Disadvantages:
The side stream sensor is placed in the main unit and not in the airway. CO2 is aspirated through a sampling tube, connected to a T piece adapter.
Advantages:
Disadvantage:
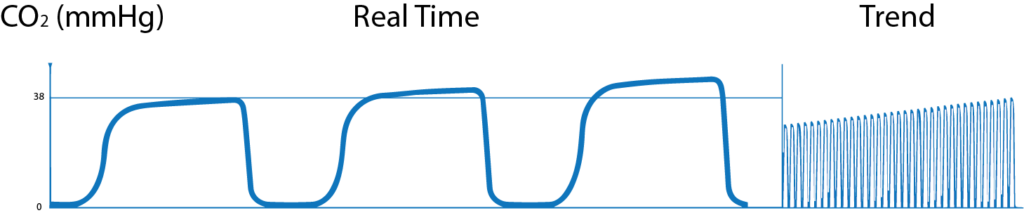
Normal Capnogram:

A-B: CO2 level is 0 mmHg. This shows the CO2 free air from dead space (Both anatomical and apparatus dead space)
B-C: In this phase, alveolar gas mixes with dead space gas, so there is steep increase in expired PCO2.
C-D: this phase is called Alveolar Plateau. Here as the CO2 rich gas is exhaled the alveoli becomes smaller and the concentration of CO2 increases towards
D: End of expiration showing End Tidal CO2.
D-E: in this phase inspiration starts and fresh CO2 free air is inhaled and so the PCO2 falls to 0.
Trend Graph: Shows changes in one hour.
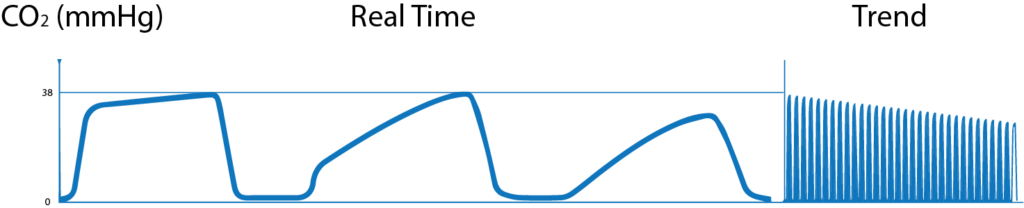
Abnormal Capnogram:
1. Gradual increase in ETCO2
2. Gradual decrease in ETCO2

3. Airway obstruction
4. Cleft in wave
5. Transient wave form

6. Distorted downward slope

7. Base line elevated and abnormal descending limb

8. Elevation of base line with corresponding increase in ETCO2

What is Capnography?, Indications, Uses and Interpretations. Read More »
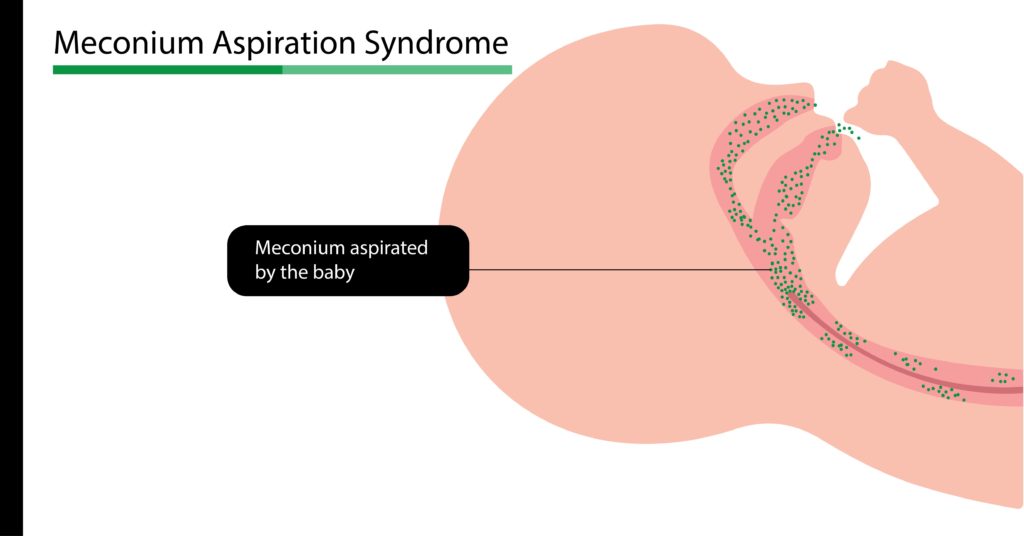
Meconium aspiration syndrome is a type of respiratory distress occurring in babies born with meconium stained amniotic fluid or aspirated meconium during delivery.
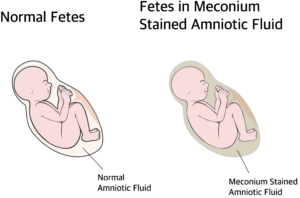
The term meconium refers to the sterile stool present in the fetal intestine. (earliest stool of the baby). Meconium contains epithelial cells of the intestine, lanugo (fetal hair), blood cells, bile, mucus, intestinal secretions and amniotic fluid. Meconium is thick, sticky, odorless and dark yellow to olive green in colour. Normally the child passes meconium hours after birth.
Passage of meconium is prevented by a low motilin level in the fetus. Motilin is a hormone (chemical) which controls motility of the intestine (peristalsis). Before delivery the motilin level will be low, preventing intestinal movements. Motilin is produced around 34 weeks of gestation. In full term and post dated babies the motilin level is high and when there is vagal stimulation by head or cord compression or stress inside uterus (hypoxia, acidosis etc) peristalsis increases and the anal sphincter is relaxed allowing meconium to come out.
This may occur during or before the delivery. Since the fetus is surrounded by the meconium stained amniotic fluid, when the baby gasps, it is aspirated into the lungs, resulting in Meconium Aspiration Syndrome.
Even though it’s sterile, it causes inflammation and may mechanically obstruct the airway, inactivate surfactant, and prevent gas exchange. Meconium aspiration syndrome is commonly found in full-term (>39 weeks) or post dated deliveries.
Depending upon the amount and duration of aspiration, the newborn may show symptoms ranging from mild to life-threatening distress. Therefore treatment has to be started as soon as possible.
What are the predisposing factors of MAS?
Mother’s:
Fetal:
Other diseases with similar clinical signs (differential diagnosis):
X-ray chest
Pulseoxymeter
To measure oxygen saturation and degree of shunting
The blood flow of the heart in the fetus is different from that of the newborn. There will be a flow of blood directly to the left side bypassing the pulmonary circulation due to high pulmonary pressure. But this becomes normal when the pulmonary pressure drops as the baby takes the first breath.
When this process is interrupted, the pressure remains high and may result in Persistent Pulmonary hypertension of Neonates. Due to this, there will be always a difference of at least 10 % SpO2 between right hand (higher than other) and other limbs.
Arterial blood gas analysis
Decreased oxygen and increased CO2, acidosis. Echocardiogram and ECG to rule out heart diseases.
Blood and aspirated meconium for culture and drug sensitivity testing.
As soon as the head is delivered, suction is applied to mouth, nose and pharynx. Soon after the delivery the baby’s vitals assessed.
If the baby is vigorous (active)
Heart rate above 100/minute, having spontaneous breathing, spontaneous movements and good tone provide supportive care with frequent monitoring. No tracheal suctioning or intubation necessary.
If the baby is not vigorous (limp)
Baby having cyanosis, increased respiratory rate, reduced heart rate and the baby is limp without spontaneous breathing, tracheal suctioning is done.
Neonatal intensive care given.
Oxygen therapy using simple oxy hood (transparent helmet-like hood) or Continuous Positive Airway Pressure (CPAP) through a mask, ECMO (Extracorporeal membrane oxygenation) or Mechanical ventilation can be started according to the severity of distress.
Empirical antibiotics to prevent infection
Nitric oxide inhalation to open blood vessels and prevent pulmonary hypertension.
Surfactant replacement therapy to replace the inactivated surfactant and open alveoli. Chest physiotherapy.
Meconium Aspiration Syndrome Read More »

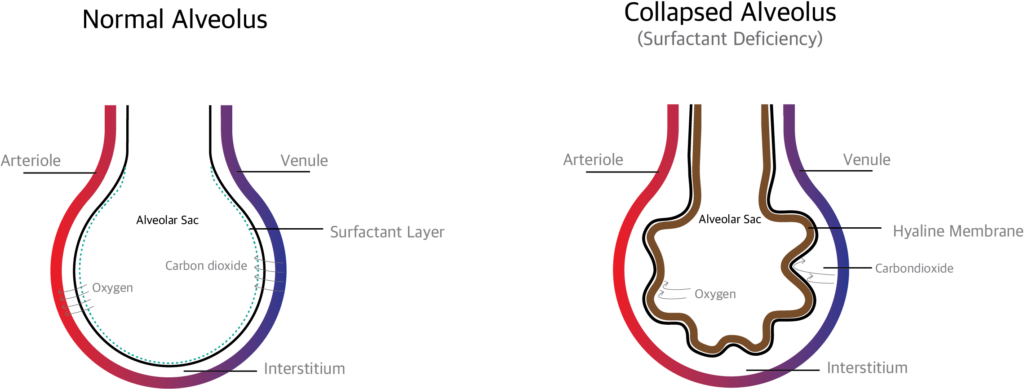
RDS once called Hyaline Membrane Disease (HMD) or Surfactant deficiency syndrome (SDD) is mainly seen in premature babies and manifest within few hours of birth due to surfactant deficiency and immature lungs. May cause death due to respiratory distress or insufficiency, if not treated on time.
The main causes are immature development of the lung and inadequate surfactant (adequate surfactant, prevents collapse of the alveoli by reducing the surface tension of the fluid lining of the alveoli).
The surfactant production starts by 24 weeks of pregnancy. In case the baby is born before this period, there is a higher chance of surfactant deficiency which leads to respiratory distress.
Normally when the baby is in mother’s uterus, the alveoli in the lung are filled with fluid. When the baby is born, the sudden change in environment and drop in temperature make the baby to take a deep breath. The fluid in the lung is reabsorbed and replaced with air.
During expiration, the alveoli is prevented from collapsing by the surfactants.. If surfactant is deficient, the alveoli collapse which in turn produces hypoxemia, CO2 retention, etc.
When the alveoli collapse the damaged cells (alveolar cells, red blood cells, white blood cells and macrophages) collect and form a membrane like structure called Hyaline membrane which prevents gas exchange.
Diagnosis can be done either prenatally (before birth) or postnatally (after birth)
Prenatal (before birth): amniotic fluid index like Surfactant / albumin ratio, Lecithin / sphingomyelin ratio and presence of phosphatidyl glycerol (PG).in amniotic fluid.
Postnatal (after birth): through clinical signs and diagnostic tests.
Oxygen saturation, Arterial blood gas analysis (ABG), routine blood investigations and blood sugar were done. X ray chest, echocardiogram and MRI chest can be done.
X ray chest shows bell shaped chest, reduced lung volume and air bronchogram Staging
Start oxygen therapy and if necessary, support respiration with noninvasive ventilation like CPAP or intubate the baby and start mechanical ventilation.
Surfactant replacement therapy: Animal derived (bovine) or synthetic surfactant can be administered through endotracheal tube. Early CPAP and surfactant administration may reduce death rate (mortality), air leak and other complications. This can be continued till the baby produces enough surfactant.
Plan of care
Supportive management includes maintaining normal body temperature, adequate fluid, acid-base balance, and proper nutrition
Prevent infections by proper vaccinations.
Respiratory Distress Syndrome (RDS) in Neonates Read More »

An arterial blood gas analysis is a procedure (test) that is performed to measure oxygen, carbon dioxide and acid/base status (pH) in arterial blood.
Arterial Blood Gas analysis is done in critically ill patients to assess the need for mechanical ventilation.
Allen’s test is done to ensure that there is good collateral circulation available from ulnar artery, if radial artery is damaged during the procedure.
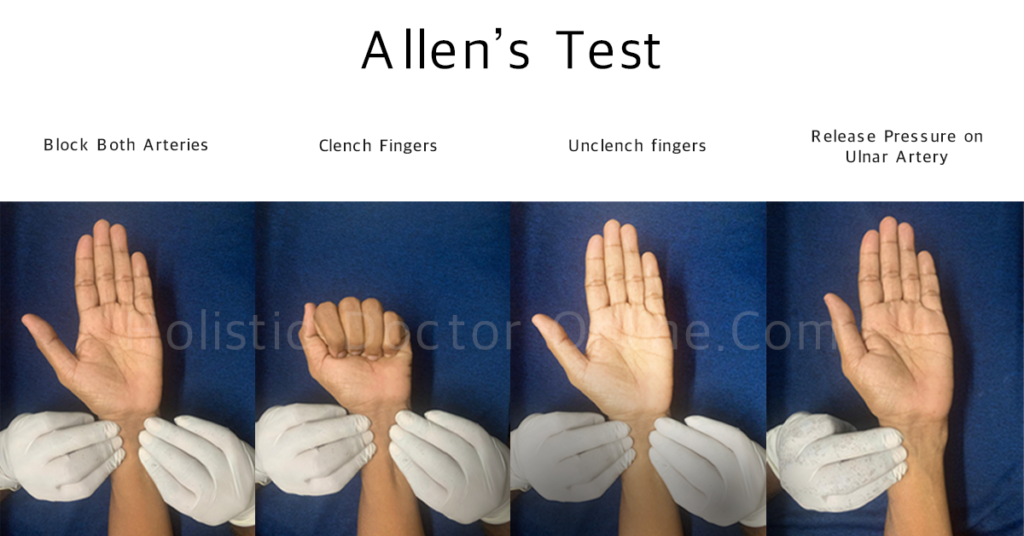
Procedure
Normal Values:
pH: 7.35 to 7.45 and absolute normal pH is 7.4.
PaCO2: 35 to 45 mmHg.
HCO3: 22 to 28 m mol/L.
PaO2 : 80 to 100 mm Hg.
SaO2 : 95 to 100%
Acidosis:
When pH is decreased, (less than 7.35)
When PaCO2 is increased (more than 45 mm Hg),
When HCO3 is decreased (less than 22 m mol/L)
Alkalosis:
When pH is increased (greater than 7.45)
When PaCO2 is decreased (less than 35 mm Hg)
When HCO3 is increased (more than28 m mol/L)
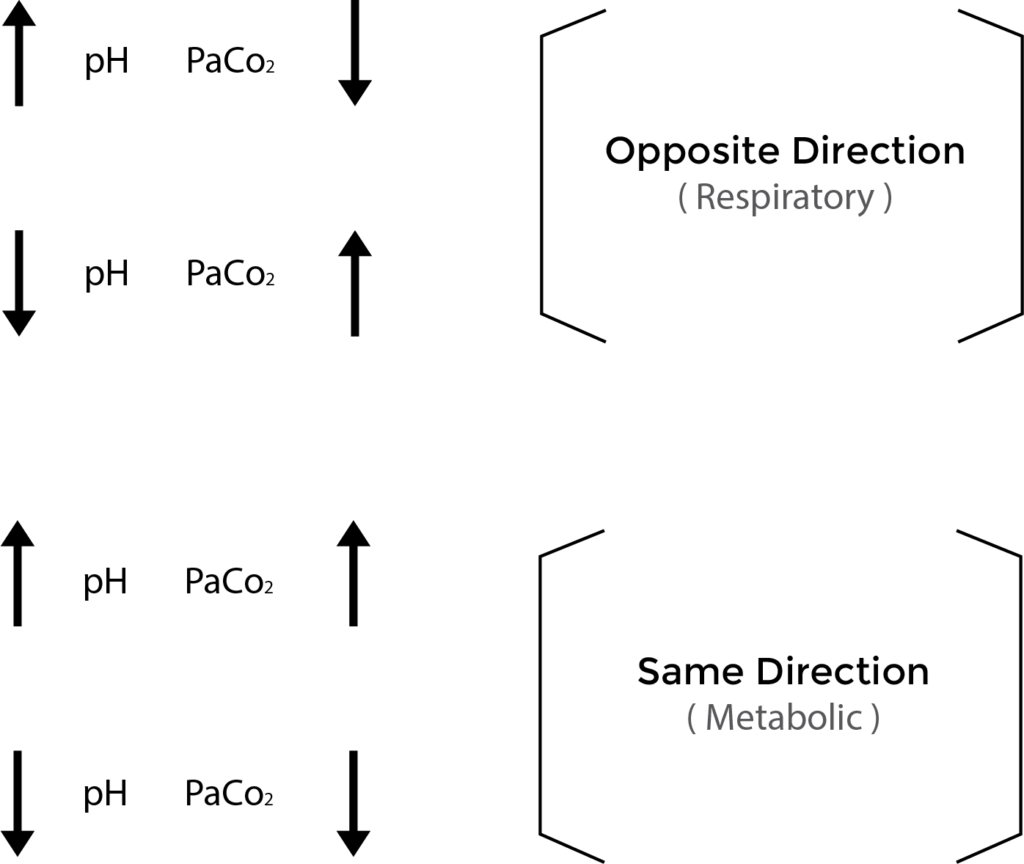
Think of ROME to know whether the cause is respiratory or metabolic.
RO: Respiratory opposite- in respiratory acidosis or alkalosis, the pH and PaCO2 values move in the opposite direction.
ME: Metabolic Equal – in metabolic acidosis or alkalosis, the pH and PaCO2 values move in the same direction.
When the chemo receptors in our body senses the change in pH, our body tries to compensate (correct and balance) it by adjusting the rate and depth of respiration or by making the kidney to adjust H+ secretion and re absorption of bicarbonate.
Example: When respiratory acidosis (low pH with high PaCO2) develops the kidneys try to compensate it by increasing bicarbonate re absorption and increase carbonic acid excretion.
Arterial Blood Gases (Arterial Blood Gas Analysis) Read More »
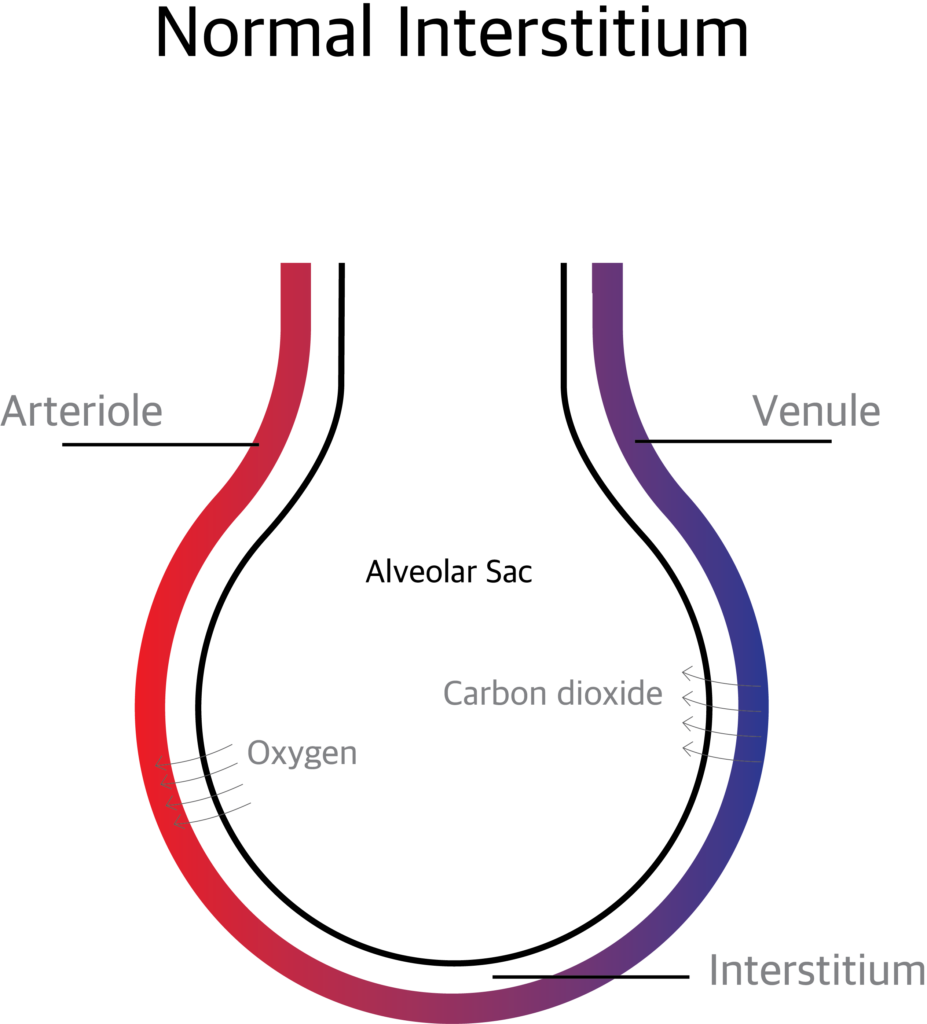
The Pulmonary Interstitium is the anatomical space between the alveolar epithelial cells and the endothelium of the pulmonary capillaries. It continues as the space surrounding the bronchi and blood vessels. The interstitium contains perivascular and peri lymphatic tissue.
The pulmonary interstitium is divided in to 3 components.
The Axial (peri bronchovascular) Interstitium: The space around the airways and the pulmonary artery.
The Parenchymal or Alveolar Interstitium: The interstitium supporting the gas exchanging part of the alveoli.
The Pheripheral or Sub pleural Interstitium: The space between the parenchyma of lung and the visceral pleura.
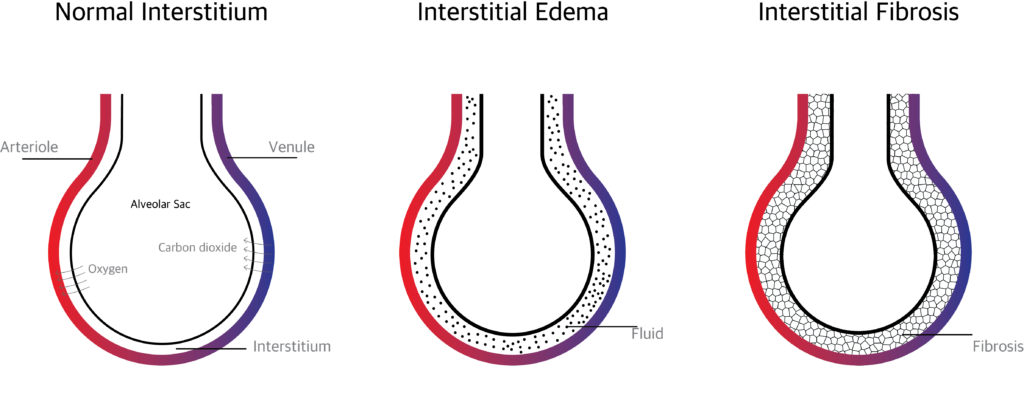
The pulmonary Interstitium supports the alveolar sacs and transport nutrients. The exchange of oxygen and carbon dioxide takes place through the pulmonary interstitium.
The gas exchange is affected when excess extra vascular fluid accumulates in the interstitium or when the interstitium is affected by inflammation and scaring.
Interstitial lung disease is a collection of more than hundred disorders affecting the pulmonary Interstitium.
Normally when there is an infection and inflammation, the interstitium will heal shortly with minimal or no scaring. Repeated insult and infection over times makes the interstitium thick and hard. This hardened interstitium becomes a barrier between the alveolar membrane and blood vessels thereby preventing gas exchange.
There are more than hundred causes. The causes may be known, unknown or hereditary.
Known Causes:
Unknown causes:
Inherited (hereditary) causes:
Symptoms:
The main symptom is gradually increasing breathlessness on exertion and finally breathlessness even at rest.
Cough usually dry, weight loss, general weakness and fever when there is super added infection.
Signs:
Digital clubbing,
Velcro crackles on auscultation.
Detailed history regarding occupation, exposure to dust, chemicals, drugs, family history, and personal history (smoking, drugs etc) has to be taken. In ILD is suspected the following investigations have to be done.
Treatment is based on the diagnosis. If due to known cause treat the cause.
If the cause is not known, the goal of the treatment should be to reduce symptoms, to improve the quality of life and to reduce complications.
Response of treatment varies. Some may recover well and some may not.
The treatment options are:
Pulmonary Interstitium and Interstitial lung disease Read More »
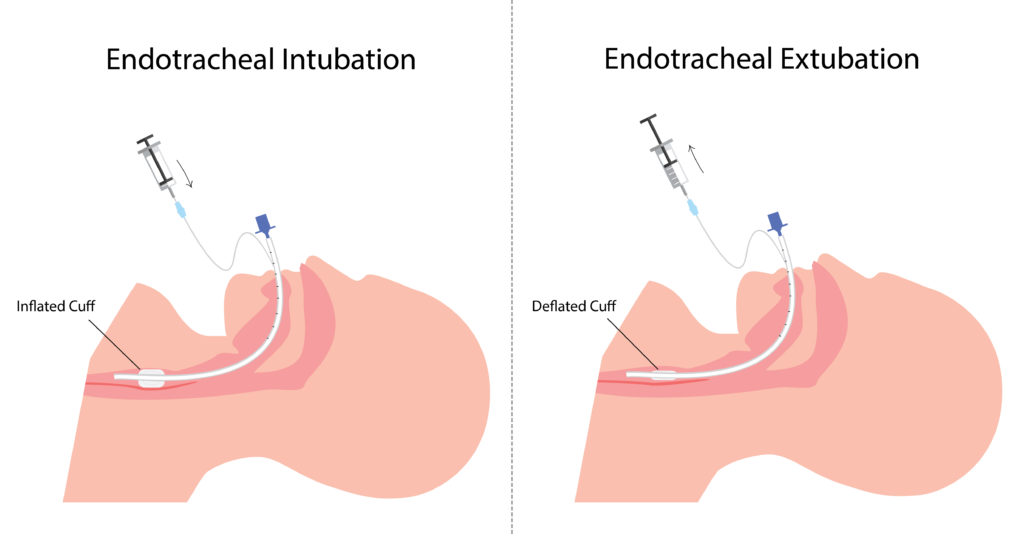
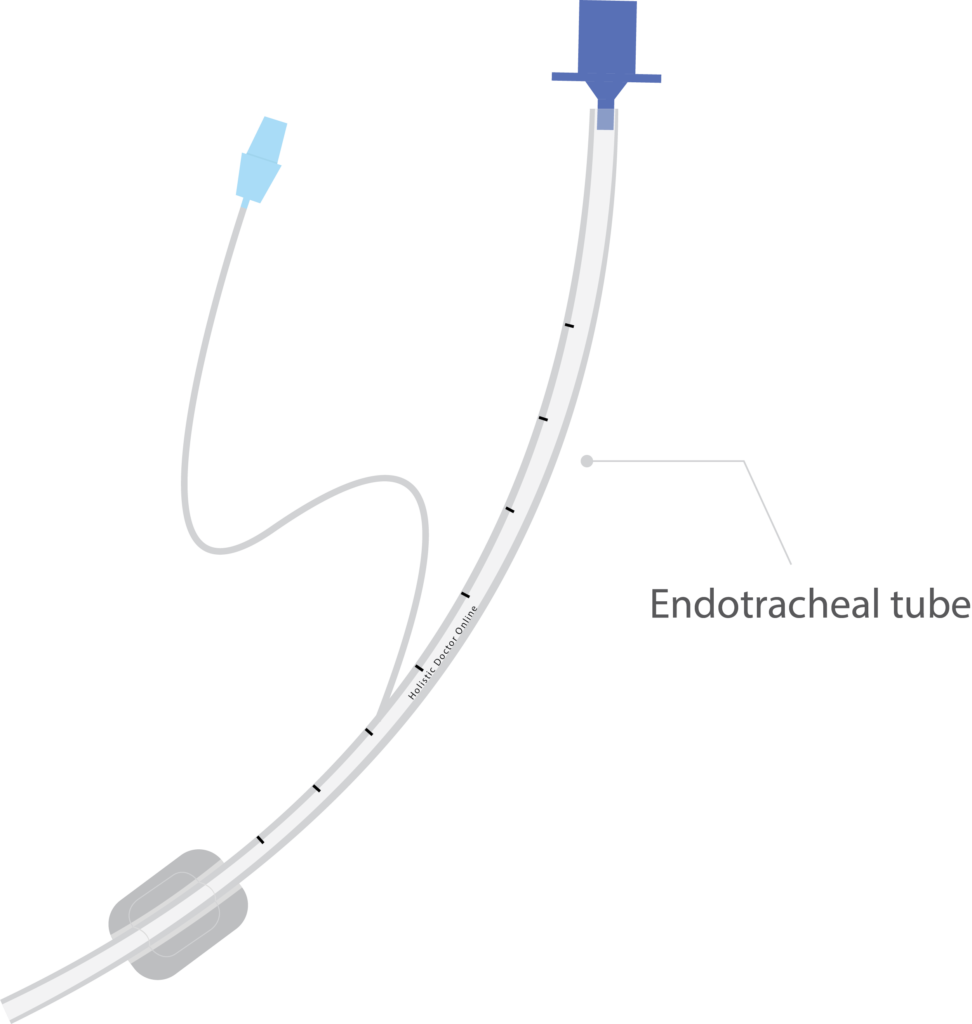
Endotracheal tube is a flexible polyvinyl chloride tube which helps to assist breathing. The process of placing endotracheal tube in the airway is called Intubation. Intubation is done to provide artificial breathing. Tracheal extubation is the process of removing the endotracheal tube from the airway.Extubation is done, once the patient is weaned (gradual withdrawal) from the ventilator.
When the patient has improved and no longer need artificial airway to breathe. If the patient is maintaining adequate gas exchange, perfusion and have improved breathing pattern and cardiovascular status.
If the patient is having improved airway protective mechanism such as cough to clear the secretions. The need for exchange of ET tube due to mucus and other secretion obstruction.
In patients who cannot maintain clear airway.
In patients who have weak respiratory muscles, inadequateventilation and perfusion.
In patients who have persistent hypoxia and hypercarbia.
In patients who have severe cardiac instability, hypothermia andmetabolic imbalance.
Before Extubation, Spontaneous Breathing Trial (SBT) is done to assess the capability of the patient to breathe in a minimum ventilatory support and oxygen support. In SBT, patient should complete 30 to 120 minutes with low level of Continuous positive airway pressure (CPAP) pressure support, showing normal breathing pattern, cardiovascular status and gas exchange.
Subjective assessment for Extubation
Adequate cough.
No neuromuscular blockers and sedatives.
Absence of excessive and thick secretions.
Improvement in disease condition.
Objective measurement for Extubation
Stable cardiovascular status.
Heart rate≤ 140 b/min.
No active myocardial ischemia.
Adequate hemoglobin levels ( ≥ 8g /dl).
Systolic blood pressure 90-160 mmhg.
Afebrile.
No or minimal vasopressor or inotrope.
Oxygenation assessment for Extubation
Tidal volume > 5ml / kg.
Vital capacity 10ml / kg.
Proper inspiratory effort.
Respiratory rate≤35minutes.
Rapid shallow breathing index<105.
PaO 2 ≥60 and PaCO 2 ≤60 mmhg.
PEEP ≤ 8cm h2O.
No significant respiratory acidosis ( PH ≤ 7.30).
Maximal inspiratory pressure (MIP) ≤‐20 – – 25 cmh2O.
O 2 saturation > 90% on FiO 2 ≤ 0.4.
Cuff leak test is done before Extubation to check the presence of laryngeal edema which is one of the major causes of respiratory failure which leads to reintubation.
Test procedure for cuff leak test
The cuff is completely deflated with a 10ml syringe and tidal volume is measured.
Cuff leak calculation ;
Tidal volume before deflation- Tidal volume after deflation= cuff leak
The percentage of cuff leak should be 15%
It low cuff leak is detected the patient has edema.
Intravenous or nebulized corticosteroids and epinephrine are administered to treat the above conditions.
All the equipments needed for the intubation must be checked and arranged, because in some cases reintubation may be required or respiratory failure may occur.
Important equipments for Extubation
Suctioning equipment
Scissors
10ml syringe
Bag valve mask resuscitator
Supplemental O 2
O 2 mask or NIV according to patients need
Crash cart
Common complications:
Hoarseness of voice
Sore throat
Cough
Other complications are,
Hypoventilation
Increased work of breathing
Respiratory muscle weakness
Aspiration due to improper suctioning
Pulmonary edema
Bronchospasm
Atelectasis
Laryngospasm
These complications of Extubation may lead to extubation failure.
When re-intubation is necessary within 24-48 hours of planned Extubation then it is called Extubation failure.
Non invasive ventilation (NIV) helps to reduce the chances of Extubation failure.
Tracheal Extubation Read More »
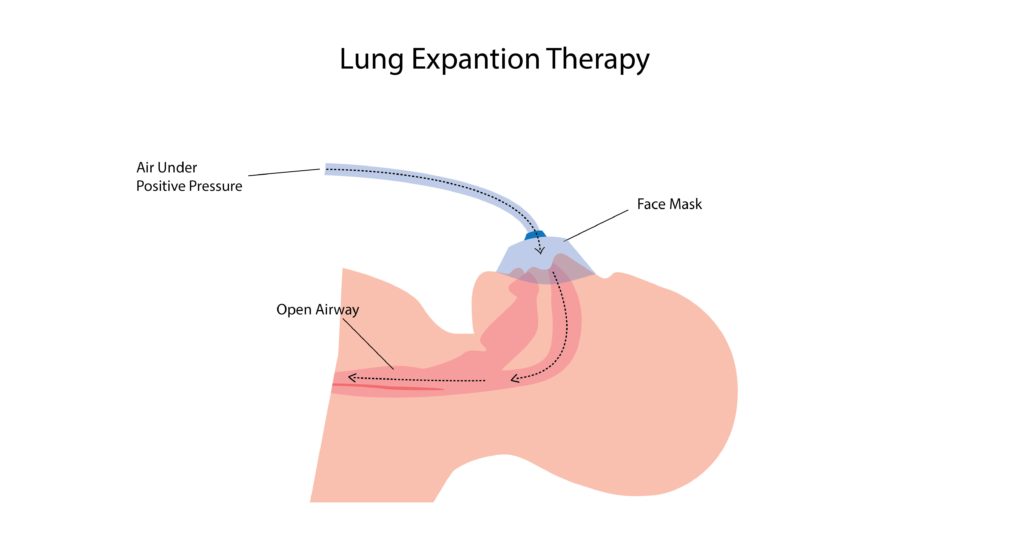
Lung expansion therapy includes many techniques to improve pulmonary function by increasing alveolar recruitment (open collapsed alveoli) and airway clearance. It increases lung volume by increasing the pressure difference between the alveolar space and pleural space (transpulmonary pressure).
Expansion of the collapsed lung can be obtained by deep breathing exercises or by applying positive pressure using devices like Incentive spirometer, CPAP, PEEP, Bi PAP, IPPB etc.
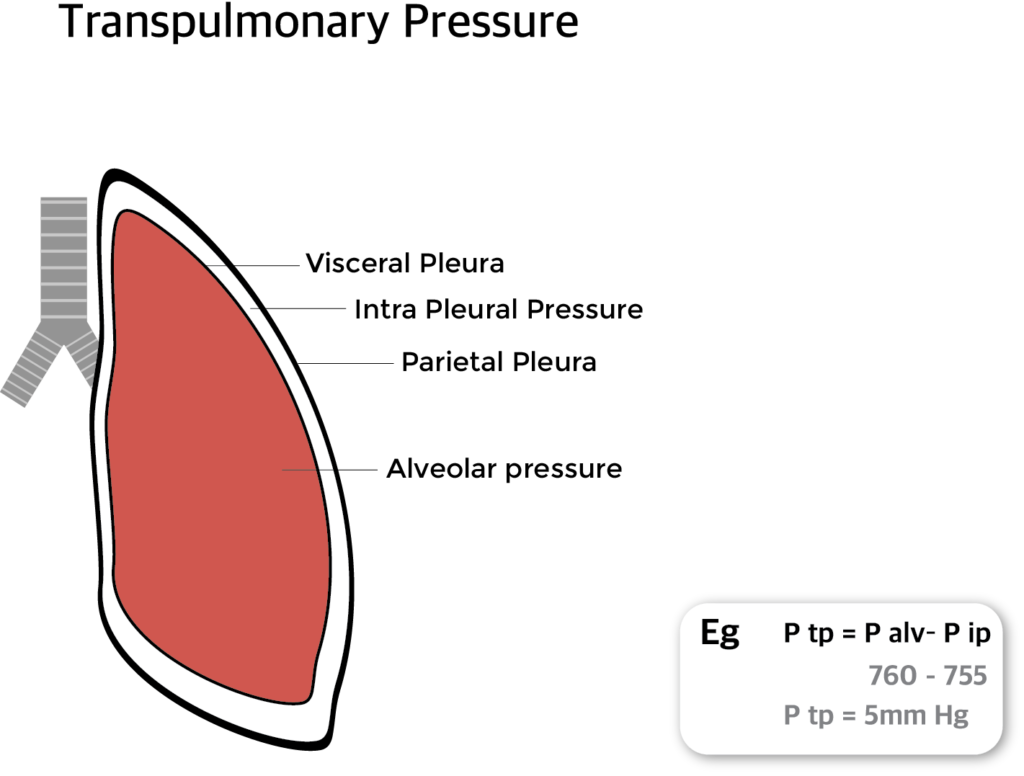
Tran pulmonary pressure (P tp) is the difference between the alveolar pressure (P alv) and intra pleural pressure (P ip).
P tp = P alv– P ip
Transpulmonary pressure can be increased by
Lung expansion therapy consists of a variety of respiratory care techniques designed to prevent or correct Collapse of lung (atelectasis).
The most common techniques include
These techniques help the patient to improve pulmonary function by increasing alveolar recruitment and airway clearance.
Incentive spirometer is a device which helps the patients to improve their lung function. The patient has to take a slow and deep breath, hold the breath for 5 to 6 seconds (sustained maximal inspiration) and then breathe out. This pressure helps to open the collapsed alveoli and airway.
IPPB (Intermittent positive pressure breathing) therapy is a technique used to expand the collapsed lung. Here inspiratory positive pressure is delivered in to the airway of a spontaneously breathing patient on an intermittent (short-term) basis by a trained respiratory therapist (RT). In IPPB a preset positive pressure is delivered only during the inspiratory phase of respiration.
This pressure helps the patient to take deep breath which in turn opens the collapsed lung and airway. IPPB is also used to improve cough mechanism, dislodge secretions and enhance delivery of inhaled medications.
In positive airway pressure therapy compressed air in a preset pressure is delivered in to the airway which keeps the lung and airways open.
It is a positive airway pressure therapy where a preset continuous pressure is maintained in the airway throughout inhalation and exhalation thereby preventing collapse of alveoli and airways.
CPAP is mainly used in obstructive sleep apnoea.
In Bi PAP therapy different level s of pressure are maintained during inspiration and expiration. Usually a pressure around 8 to 12 cm of water (H2O) is maintained during inspiration and pressure around 2 to 4 cm of H2O is maintained during expiration.
Bi PAP is a type of non invasive type of mechanical ventilator. It is usually used in patients with COPD and patients with respiratory distress and in Obstructive Sleep Apnoea patients where CPAP is not effective.
In PEP (Positive Expiratory Pressure) Therapy the patient is made to breath out (Exhale) against resistance through a PEP device. The pressure created is transmitted to airways, creating a back pressure which prevents collapse and keep the airways open during exhalation.
PEP therapy prevents collapse of lung and airways, prolong expiratory flow and promote airway clearance.
Patient has to inhale, hold the breath and exhale through the PEP apparatus. A pressure around 10cm of water is maintained at mid expiration.
EPAP (Expiratory Positive Airway Pressure) therapy works by creating pressure during expiration and keeping the airway open until n inspiration. It is a simple, non invasive and effective treatment for obstructive sleep apnoea.
EPAP device consists of 2 two way valves one for each nostril. On inhalation the valves open and allow air to enter freely and on exhalation the valves restricts air flow. This restriction increases pressure inside the airway and prevents collapse of airway.
The EPAP device is small, portable, not attached to any machine and no need for power supply. Airway Pressure (EPAP) which is maintained until the start of the next inspiration.
Lung Expansion Therapy Read More »
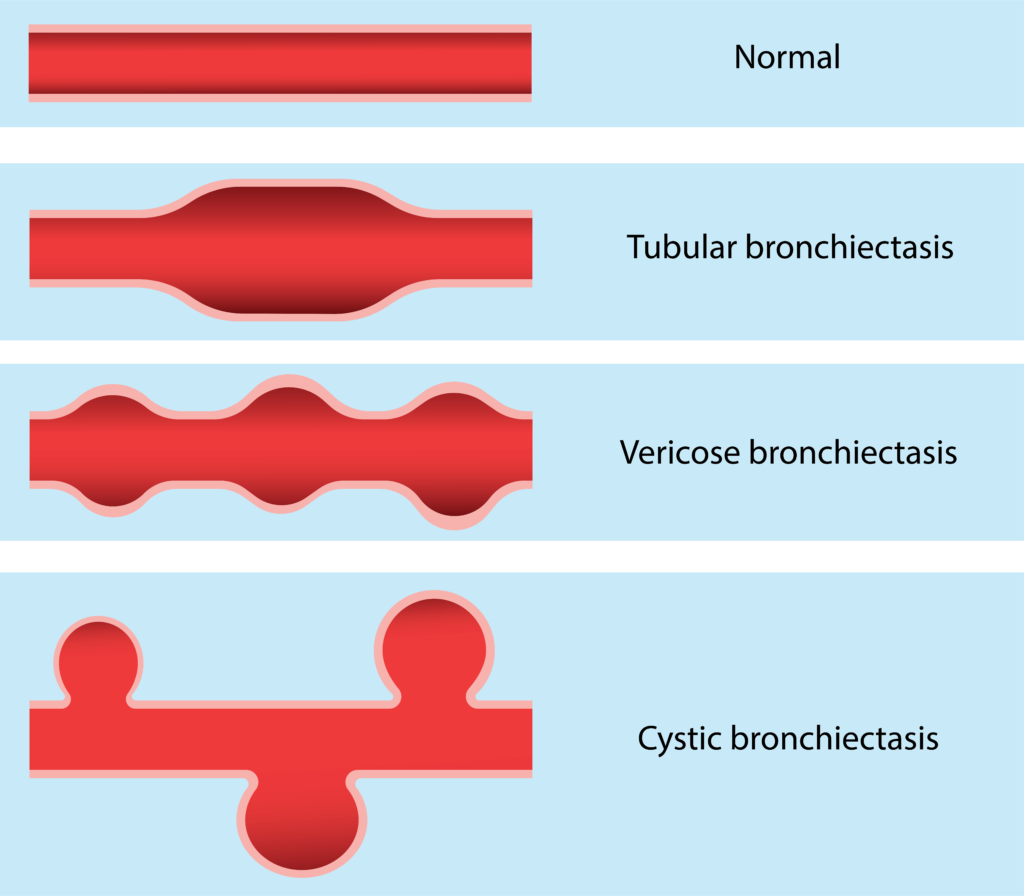
Bronchiectasis is an abnormal irreversible (permanent) dilatation of some bronchi or bronchioles (enlargement of parts of airway).
The main cause of bronchiectasis is frequent, chronic lower respiratory tract infections like tuberculosis, haemophilus influenza, streptococcus, klebsiella etc. Bronchiectasis can occur as a complication of Cystic Fibrosis. A congenital (hereditary) condition called Kartageners syndrome where there is defect in ciliary function can also produce bronchiectasis.
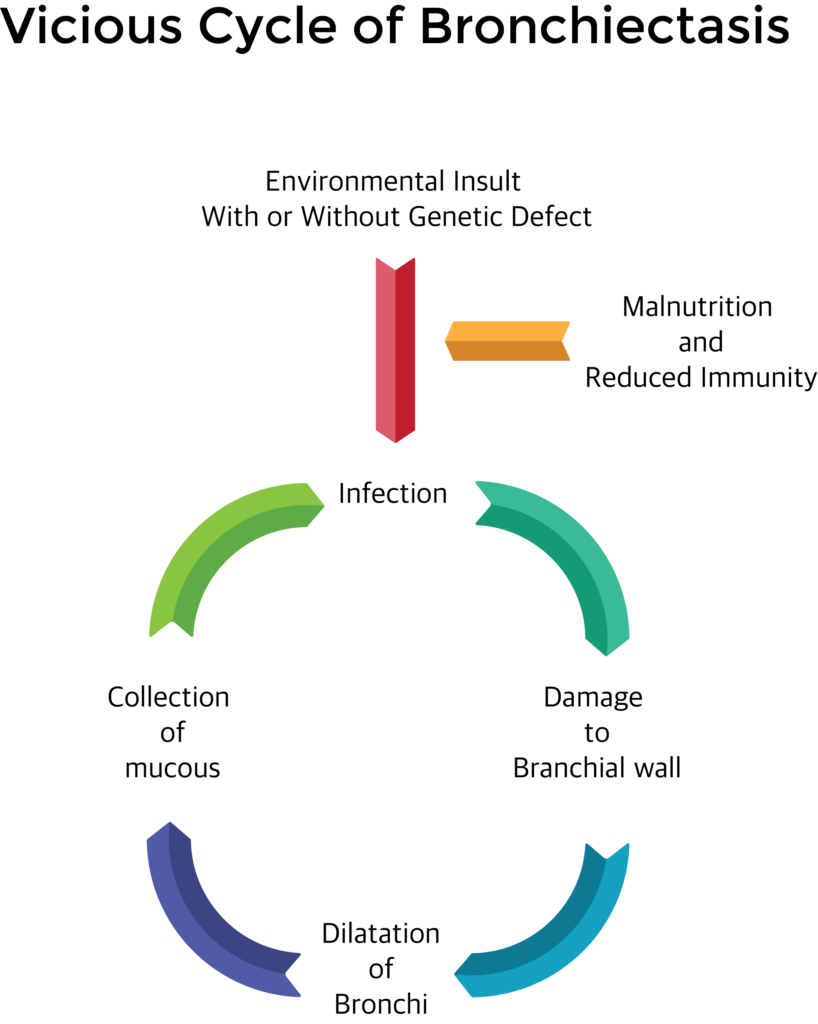
Chronic infections may damage the mucosal layer and mucociliary clearance. Inflammatory cells infiltrate leading to sloughing and ulceration in the wall of the bronchi. This may lead to patchy scarring and dilation of the area of bronchi. In the dilated area mucous gets collected which in turn gets infected and produce further damage.
According to the shape of dilatation, there are three types of bronchiectasis. They are cylindrical, tubular and varicose.
Symptoms
Signs
X ray chest: increased bronchovascular markings, multiple cysts containing fluid levels.
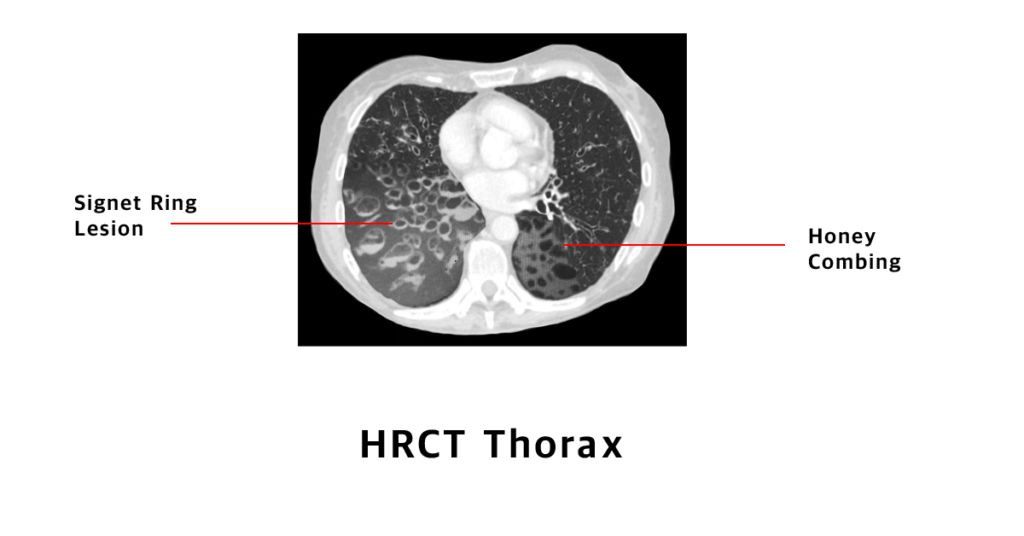
HRCT scan chest: Signet ring lesions, honey combing with fluid levels.
Sputum test for gram stain and acid fast stain.
Sputum for culture and drug sensitivity testing,
Routine blood tests like bloodcount, ESR, Bloodsugar,
Bronchography or bronchoscopy.
Postural drainage and chest physiotherapy.
Antibiotics: Start with broad spectrum antibiotics and can be changed according to the drug sensitivity.
Bronchodilators and expectorants,
Airway clearance devices,
Reassurance and health education.
Surgical excision: Very rarely done when bronchiectasis is localized and with severe haemoptysis.
Diagnose and treat respiratory tract infections early.
Vaccinations schedule to be followed in children and adults can take pneumococcal vaccine like PISV 23 or PCV 13.
Prevent malnutrition by taking well balanced high protein diet.
Causes, Symptoms, Diagnosis and treatment of bronchiectasis Read More »
Respiratory therapist also called as respiratory care practitioners are paramedical professionals who basically deals with the problems related to lungs and airways of an individual from their first breath till the very last breath i.e., all age group of patients who has a simple cough or someone who require I.C.U care. The Respiratory Therapist can help them as an individual or as a part of multidisciplinary team to improve the health related quality of the patient.
Respiratory Therapist can work in coordinate with physicians in order to formulate individual care for patients depending upon their respective disease condition i.e., in co-ordination with Pulmonologist, Pediatricians, Anesthetist, Critical Care Medicine, Emergency Medicine, or even in pre and post operative care as a backup for Surgeons to restore ventilation. In a hospital, they can work in outpatient department, inpatient department, critical care unit, pulmonary rehabilitation centre and pre or post operative care unit.
The vital role of Respiratory Therapist is to assess, aid in diagnose or treat and care for patients with cardiopulmonary disorders. They play a vital role as a member in Code blue team (Cardio Pulmonary Resuscitation) to restore ventilation to the lungs, which includes a vast category of patients from newborns to elderly.
Respiratory therapist takes a brief history of patients, perform some physical examination and also help in diagnosis of the patient’s disease with the help of certain equipments.
Respiratory Therapist generally work around 35-40 hours a week. Depending upon their work place this time may vary. Average salary ranges around Rs 18,000- 25,000/ month depending field of interest and work area.
Most of the Respiratory therapists must complete a 2-4 year program of study and can register in IARC (Indian Association of Respiratory Care). In short Respiratory Therapists provide both temporary relief and permanent solution to patients suffering from disorders related to lung and airways of all age group. The goal of the respiratory therapist is to help the patient to breathe with comfort.
Respiratory therapist Read More »
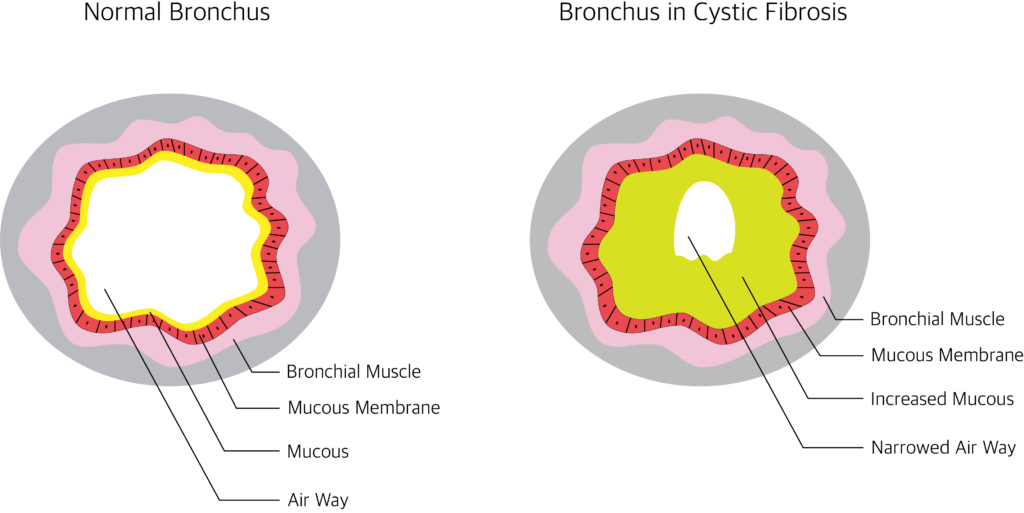
Cystic Fibrosis is a hereditary disease caused by gene mutation (alteration in gene sequence and structure). The mutation occurs in the gene for the CFTR protein (cystic fibrosis Trans membrane Conductance Regulator) on chromosome 7.
The main feature of Cystic Fibrosis is an abnormal high level of sodium and chloride in secretions of exocrine glands.
Cystic Fibrosis is seen in new born babies and seen in 1 in 2000 live births.
Cystic fibrosis mostly affects the lungs. It can also affect secretory organs like sweat glands, digestive system, pancreas and liver.
Because of the abnormal composition of sodium and chloride the mucus becomes thick and sticky. This impairs the mucociliary clearance. This leads to chronic infections and further leads to bronchiectasis, emphysema etc.
Respiratory system
Other organs
In neonates: Meconium ileus, failure to thrive, rectal prolapse and distended abdomen.
In adults:
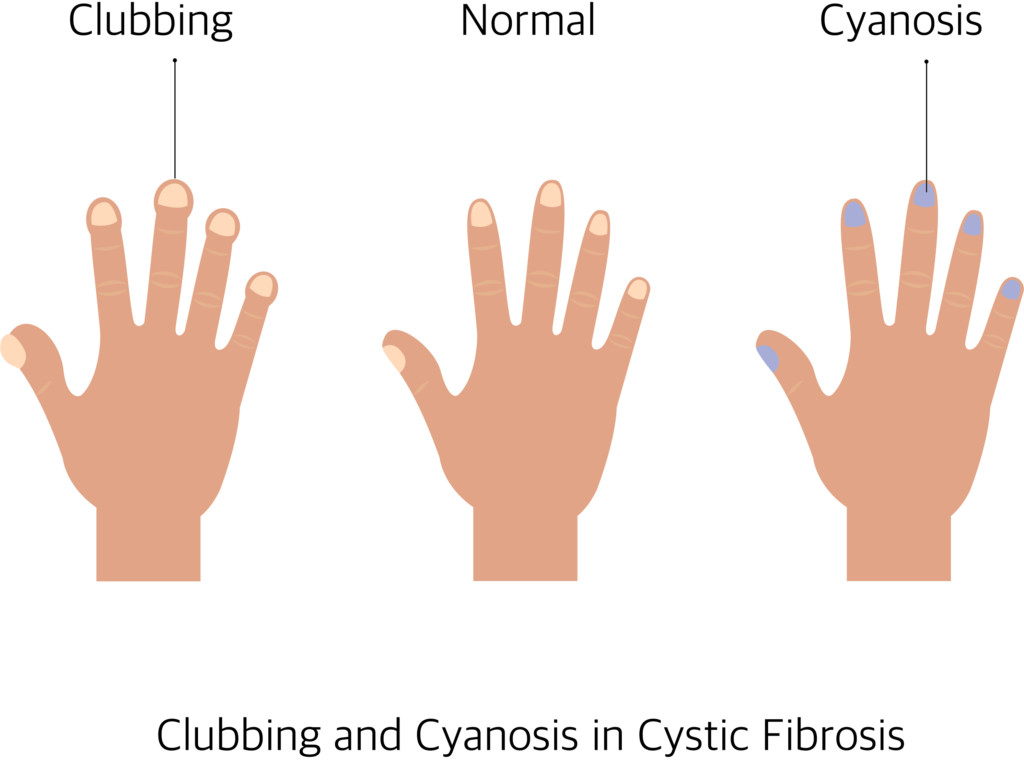
Clubbing: Tips of toes and fingers are enlarged.
Cyanosis: Bluish discoloration of nail, lips and tongue.
Bilateral coarse crackles heard over lung field.
Cystic Fibrosis cannot be cured completely. Treatment is aimed to reduce symptoms, slow down the progress of cystic fibrosis, prevent complications and to improve the quality of life.
Following treatments are given:
Cystic Fibrosis can’t be prevented. Avoid marrying people with family history of Cystic Fibrosis. If parents have cystic fibrosis in their family, genetic testing can be done through amniocentesis (Remove fluid from the pregnant uterus) to rule out cystic fibrosis in the unborn baby. Genetic counselling before marriage is done to prevent producing babies with cystic fibrosis.
Cystic Fibrosis Causes, Signs, Symptoms and Treatment. Read More »
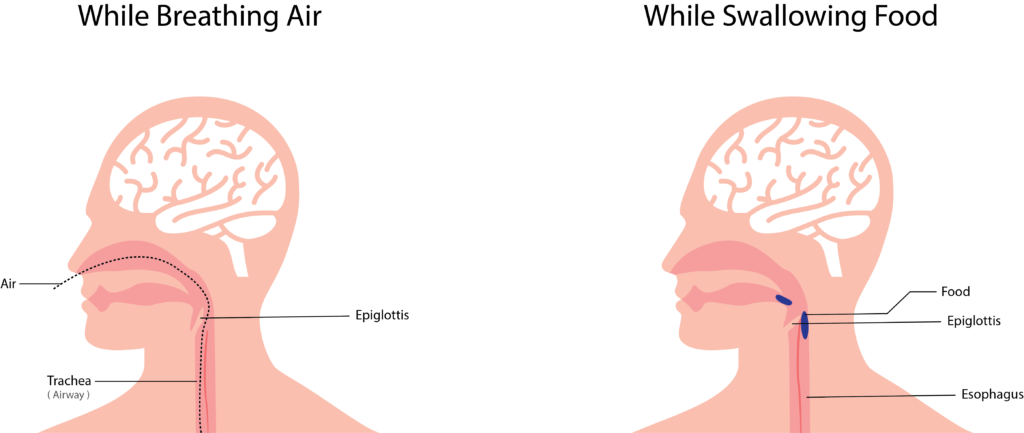

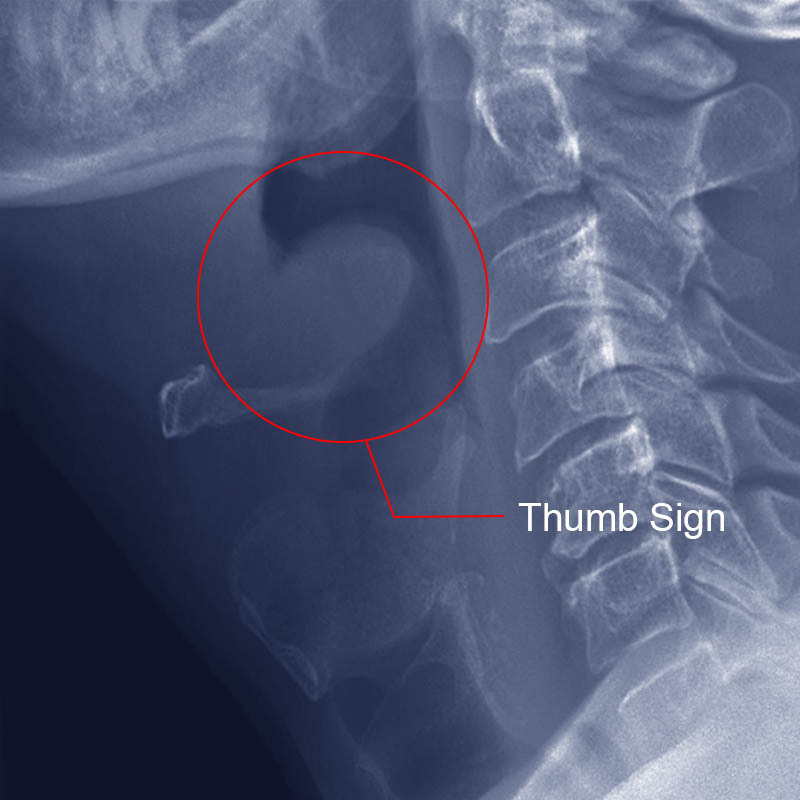
Epiglottitis is the swelling (inflammation) of the epiglottis.
Enlargement of epiglottis may lead to blockage of upper airway by blocking the entry of air during respiration.
It usually causes breathlessness and blockage of windpipe. It is a medical emergency and may lead to death if proper treatment is not initiated immediately.
Epiglottitis usually affects children, but it can occur at any age. Epiglottitis affects non immunized and malnourished people.
Dyspnoea: difficulty in breathing,
Dysphagia: difficulty in swallowing,
Dysphonia: difficulty in speaking (voice disorder),
Drooling: dribbling of saliva.
What is Epiglottitis ? Causes, diagnosis and treatment of epiglottitis Read More »

Intubation ( Endotracheal Intubation ) is a process of placing a tube in the airway from the nose or mouth to trachea (wind pipe) to provide artificial respiration.
Intubation is done in patients with conditions such as respiratory failure, cardiac arrest, trauma etc.
Intubation is done in patients who cannot maintain a clear airway, who have severe airway obstruction and in patients who are unable to breathe on their own. It is also done to give general anesthesia and to start mechanical ventilation.
Intubation procedure must be carried out by well-trained medical professionals like doctors, respiratory therapists etc . Intubation is done in emergency conditions in ICU and operation rooms.

Before intubation the equipment’s must be checked and assembled. ET tube and laryngoscope must be selected according to patient’s size.
Before intubation ET tube must be checked for cuff leaks, it must be inflated and deflated with syringe. Bulb, blade, battery must be checked in the laryngoscope. Other equipment’s such as syringe tongue depressor, sty let, tapes, and Magill forceps must be checked and assembled.
Yankaeur suction can be used for oral suctioning. Vacuum pressure should be checked before suctioning. Suctioning is the process of applying negative pressure to remove the secretions and fluids in the airway. Before intubation patient should be 100% oxygenated with bag mask ventilation.
No intubation procedure must exceed 30 second. If intubation is not done within given with 30 second the oxygenation should be given with bag mask ventilation for 3 to 5 minutes.
In elective procedures, patients must be kept on fasting (no food or water) for a minimum period of 6 hours to prevent aspiration of food materials in to respiratory tract.
For conscious patients sedation must be given to reduce anxiety. Patient is paralyzed to prevent resistance and to prevent vomiting. Local anesthetic is sprayed to numb the throat.
The medical professional doing intubation must stand behind the head of the patient. The patient must be in lying position. Sniffing position is done during the intubation; it is done by flexing the neck and tilting the head backward using hands. The sniffing position aligns patient’s mouth, pharynx and larynx in a same line and it opens the airway which helps in better visualization for the ET tube insertion.
The laryngoscope is an instrument which contains a holder and blade. It helps in better visualization of larynx. It consists of two types of blade – Miller (straight blade) and Macintosh (curve blade).
The medical professionals must use left hand to hold the laryngoscope and the right hand to open the mouth and to insert the tube. The laryngoscope must be inserted from the right side of the mouth; the tongue must be displaced to the left. The laryngoscope must be preceded until the visualization of epiglottis.
The epiglottis must be moved for the insertion of ET tube. Moving the epiglottis gives better visualization of vocal cord where the ET tube is inserted. Epiglottis is present at the entrance of voice box; this prevents the entry of food particles into the wind pipe. It opens during breathing, cough and sneezing etc.
The curve blade is positioned at the base of the tongue the laryngoscope is lifted up and forward for moving of epiglottis. The straight blade is positioned posterior to epiglottis were the laryngoscope is lifted up and forward for moving epiglottis. If the glottis is visualized the ET tube must be inserted from the right side of the mouth. The ET tube should be passed inside the airway until the cuff enters the vocal cords.
Stylet must be used for a stiff placement of ET tube. ET tube is passed easily if water soluble jelly is applied over the tube. Once the ET tube is inserted in the airway laryngoscope and stylet must be removed.
The cuff should be immediately inflated with a 10ml syringe. The cuff helps to maintain the tubes position in the wind pipe and also prevents the entry of foreign particles into the lungs. The ET tube must be placed 3 to 6 cm above the tracheal bifurcation (division of trachea).
Chest wall movements – After ET tube placement bag mask ventilation should be done. If bilateral chest wall movement is observed the ET tube is located above the carina. If abdominal bloating is observed, the ET tube is placed in the food pipe and re intubation should be done in this condition.
Bilateral lung sounds – Auscultation is done to check the bilateral lung sounds. If no lung sound isobserved in the left lung the ET tube is placed the right main bronchus. In this condition the ET tube must be slightly pulled out. If there is absence of lung sound the ET tube is in the food pipe. Reintubation should be carried out.
Bronchoscopy: This procedure shows the accurate position of the ET tube.
Capnometry: It is the measurement of CO 2 in the exhaled air. Normal PCO 2 in the exhaled air is 35 to 45mm of hg. If less amount of CO 2 is indicated the ET tube is in food pipe and re intubation should be done in this condition.
Chest x-ray: The radiograph line present in the ET tube shows the position of ET tube in the airway.
Tube length: The length marking present in the ET tube is used to determine the positioning. The tube length from the teeth to the tip is used to rule out the depth of the ET tube in the airway.
After confirmation of the ET tube placement in the airway it is held in position with tapes or tube holder. Oropharyngeal airways are placed to prevent the tongue fall back & to prevent the biting of tube. Then the ET tube is connected to the ventilator.
When the patient is weaned from mechanical ventilator and the patient cab breath on his own, ET tube can be removed. The adhesive tape holding the ET tube to the face is removed, the cuf of the Et tube is deflated and the ET tube is slowly pulled out.
Intubation can produce tissue damage, bleeding, improper placement leading to cerebral ischemia and brain damage. It can damage the larynx and vocal cord and produce speech problems. Intubation can also produce tracheal stenosis, tracheooesophageal fistula, pneumothorax, atelectasis and infection.
Endotracheal Intubation Read More »

Pneumonia is the inflammation of the lung parenchyma ( tissue that involves in gas exchange in the lungs otherwise called alveolar tissue ). When inflammation is caused by infection it is called pneumonia and when inflammation is caused by other causes like radiation, inhalation of chemicals etc… it is called as pneumonitis.
Pneumonia can be caused by infection, inhalation of chemicals and gas or by aspiration of foreign bodies.
Pneumonia can be classified according to
1. The anatomical site involved
2. The Source of infection

3. The organisms causing
X-ray Cheat, HRCT Thorax, Sputum examination: Gram stain and AFB stain, Sputum culture and sensitivity, Blood culture, Serological tests for viral infection and to rule out HIV infection, Routine investigations like CBC, blood sugar, urea and creatinine.
Prognosis can be assessed using CURB-65 scoring system.
One point is given for each.
C – Confusion
U – Urea: more than 7 m mol/L
R – Respiratory rate: more than 30/ minute
B – Blood pressure: less than 90 systolic and/ or 60 diastolic.
65 – Age above 65.
Severity
If the total score is
0 to 1 – Mild outpatient treatment is enough.
2 – Hospital admission necessary.
3 to 5 – Severe, intensive treatment necessary, the death rate increases as the score.
Mild patients can be treated as outpatients with oral antibiotics and antipyretics. Moderate and severe patients need injections and intravenous fluids with oxygen support. Severe patients may need mechanical ventilation.
Broad spectrum antibiotics are started and later on altered according to the culture and sensitivity report.
Fever, body pain and other symptoms can be treated accordingly.
Pneumococcal vaccine (like 23 valent pneumovax) can be given to vulnerable people like senior citizens over 65 years, diabetics, patients with pre existing lung disorders or patients on immunosuppressant drugs.
Pneumonia: Symptoms, Causes, Treatment and Prevention Read More »
Article written by Ravindran O.S & Aruna Mani
Internet addiction is characterized by excessive use of the internet, and that is detrimental to the user. There exists no clear definition for internet addiction as there is lot of uncertainty and disagreement among experts about overuse of the internet, the symptoms, how to measure it and even the language used to describe it as explained by the American Psychiatric Association. An American psychiatrist Jerald Block, (2008) stated that there exists three types of internet addiction: excessive gaming, sexual preoccupations, and email/text messaging, and all three types share four components: excessive use, withdrawal, tolerance for the costs of the activity and negative repercussions.
A foremost expert on Internet Addiction Disorder, Young (2011) grouped internet addiction into six subtypes which are as follows:
Many research studies conducted in the past reveal the strong association between internet addiction and personality traits. Previous studies found a positive association between problematic internet use and interpersonal problems such as social skill deficiency, loneliness and social anxiety (Caplan, 2005, 2007., Morahan-Martin and Schumacher, 2000, 2003.,). Similar findings from another study revealed shy people or those disappointed by real relationships exhibit a certain behavior style which aims at finding a way to reach the outer world so that they are able to control it (Morrison and Gore, 2010). Impulsive behaviours (Reed et al, 2015), loneliness, alexithymia and suicide (Alpasla, et al, 2015) are also associated with excessive internet use. In young adults, social anxiety has been linked with internet addiction (Weinstein, et al, 2015), lower levels of family functioning, life satisfaction, and problems in family interactions (Wartberg, et al, 2015). It was also found to give rise to incidences of substance use, poor emotional well-being, and decreased academic performance in adolescents (Rucker, et al, 2015) and increased academic stress (Jun & Choi, 2015). People found to be higher in narcissistic personality traits tend to be more active on facebook and other social networking sites in order to present themselves favourably online because the virtual environments empowers them to construct their ideal selves (Buffardi & Campbell, 2008; Mehdizadeh, 2010).
Diagnostic assessment of Internet Addiction Disorder proposed by Beard (2005) is widely accepted. He proposed five diagnostic criteria in the identification of Internet Addiction Disorder in the general population which are as follows:
In addition, Beard suggested at least one of the following must be present in a diagnosis of Internet Addiction Disorder:
Effects of internet addiction can manifest as physical or emotional. Some of the common emotional reactions are feelings of guilt, dishonesty, difficulty in keeping up with deadlines, poor time management, isolation, avoidance behavior, and agitation. Some of the physical effects manifested include headache, weight loss or gain, sleep disturbances, backaches, vision problems, and reduced self-care. Prolonged internet addiction has also been observed to have correlation with psychiatric and psychosocial conditions. Some of the commonly observed conditions are low self-esteem, impulsivity, poor sleep quality, mood disorders, suicide, ADHD, social phobia and depression, and in some cases even leading to loss of job, bankruptcy, and failed relationships.
Internet addiction, though is not an official diagnosis in the Diagnostic Statistical Manual, however, it is believed to share similarities with impulse control disorders and gambling addiction. Treatment for internet addiction argued by some authors indicate that total abstinence from the internet should not be the goal of any intervention, and that instead an abstinence from problematic online activities and regulated use of the activity should be achieved (Cash H, et al. 2012, Khazaal Y, et al. 2012). However, more empirical evidence is needed to validate such claims. In terms of psychological treatment for internet addiction, cognitive-behavioral therapy is the most influential.
References
Internet addiction: a review of its conceptualization, prevalence, neuronal processes, and implications for treatment. Neuroscience and Neuroeconomics. 2015. 4, 11-23. doi: https://doi.org/10.2147/NAN.S60982
Big five-personality trait and internet addiction: A meta-analysis review. Computers
in Human Behavior
Internet addiction Read More »

Dark circle under the eye is one of the common cosmetic problems faced by both men and women. It may make them appear older and it gives them a hollowed –out look (ghost like look).
Dark circle under the eye can be caused by a combination of causes.
The causes are:
Over Exhaustion, Overstraining and tiredness can produce dark circle under the eye.
Physical Stress, mental stress, Sleep deprivation (Not getting enough sleep) and rubbing the eyes vigorously can produce dark circles under the eyes.
Dehydration (not drinking enough fluids) can also produce dark circles.
Ageing, genetic conditions and hormonal imbalance can cause dark circles under the eyes.
Anemia (Iron Deficiency), Vitamin Deficiencies, and malnutrition can cause dark circles under eyes.
Allergies and skin diseases can also produce dark circles.
Over exposure to sunlight, Using inappropriate eye glasses, refractive errors of the eye and overstrain of the eye (like using computers or mobile phones for long without rest) can cause dark circles under the eyes.
General Treatment:
Good rest to the eyes. Eight hours of sleep, Reduction of stress, Eating a well balanced diet with lots of green leafy vegetables and fruits and Drinking lots of fluids can prevent and reduce dark circles under the eyes.
LEMON JUICE: Applying lemon juice over the dark circles and washing it off with cool water after 20 minutes can reduce dark circles.
CUCUMBER: Keeping slices of cool cucumber over the eyes and taking rest for 20 minutes or applying cucumber juice over the dark circles and washing it off after 20 minutes reduces dark circles under the eyes.
POTATOES: Cool potato slices kept over the eyes or applying cool potato juice over the dark circles and washing it off after 15 to 20 minutes helps to reduce dark circles under the eyes.
Applying a mixture of lemon juice, potato juice and cucumber juice over the dark circles and washing it off after 20 minutes gives better and faster results.
MILK: Milk moisturizes and lightens the skin. Applying cotton pads soaked in cold milk over the dark circles and washing it off after 30 minutes gives good results.
GREEN TEA: Refrigerated & soaked green tea bags can be kept over the eyes for15 minutes to reduce dark circles.
Tomato juice, Coconut oil, Honey, Almond oil, Vitamin E, Turmeric powder, mint, licorice extract or baking soda can be applied over the dark circles and washed after 15 to 20 minutes can reduce dark circles under the eyes.
Other Treatments Available:
LASER THERAPY: Sending burst of laser light to Dark circles may tighten the skin and allow growing new lighter skin.
CHEMICAL PEELS: Chemical peels using Retinoic acid or Hydroquinone help to reduce dark circles.
Intense Pulse Light Therapy (ILP) and Plastic surgery can also be used to treat dark circles under the eyes.
The dark circles can be camouflaged or concealed with makeup.
To prevent dark circles under the eyes take nutritious well balanced diet.
Avid smoking, excessive alcohol, and late night parties. Look away from computer or mobile screen every few minutes. Have minimum 8 hours of good sleep.
Avoid over exposure to sun light. Use sun screen when going out in hot sun. Use dark sunglasses prescribed by doctors.
Drink lot of fluids like fruit juices and tender coconut water when going out in hot sun to prevent dehydration.
Dark circle under the eye Read More »